
Published in hbvadvocate.org
December 30, 2010
By Christine M. Kukka
A potential new, powerful treatment for hepatitis B, treating pregnant women to prevent infection of newborns, increased political and medical awareness of hepatitis B, and health care reform provisions have all had an impact on the hepatitis B community during 2010.
Three years ago, there were far fewer articles, studies and reports about monitoring, treating and preventing hepatitis B. This year, numerous studies and clinical trials have tracked the effectiveness of antivirals and interferon, and researchers have come up with new methods to monitor liver health, and screen those at risk of hepatitis B virus (HBV) infection.
Here are some of the major discoveries, reports, and public health initiatives that have had an impact on hepatitis B worldwide in 2010:
A National Model Emerges to Screen and Treat Asian-Americans for Hepatitis B: In 2007, community organizers in San Francisco began organizing the Hep B Free Campaign to increase screening, treatment, and immunization for hepatitis B. The initiative, which started with minimal funding, now involves more than 50 public and private health care organizations, businesses, and educational institutions, as well as Major League Baseball's San Francisco Giants, and has become a national model for increasing access to health care for those at risk of HBV.
The campaign, focusing on a city that has the highest rate of liver cancer in the country, has created seven low-cost public access hepatitis B screening and vaccination sites through collaboration with community partners, public and private hospitals, doctors, insurance and pharmaceutical companies, and non-profit organizations.
San Francisco, with its high percentage of Asian-American residents, has the highest rate of liver cancer in the nation and is the gateway for immigrants from Asian countries where there is a high prevalence of hepatitis B. The model is now being copied in San Mateo, San Jose, Orange County and Los Angeles, and federal and state health officials are touting its success and suggesting it be used in other cities with at-risk populations across the country.
Activists Utilize Provocative Social Marketing to Fight Hepatitis B: For years, critics have faulted hepatitis B activists for their low-profile, under-the-radar efforts to raise awareness of hepatitis B among those at risk for the infection, particularly Asian-Americans. Unlike AIDS activists, who publicly acknowledged their infections and staged public protests to raise awareness and push for fast-track development of AIDS drugs, hepatitis B organizers have been quiet, in part because many Asian-Americans found the culture of public protest and discussion of illness and death distasteful.
As part of San Francisco’s Hep B Free campaign, the Asian-American advertising agency DAE produced a provocative ad campaign entitled “Which One Deserves to Die” to alert the public that 1 in 10 Asian-Americans is chronically infected with HBV.
The posters appeared in local ethnic and mainstream newspapers, billboards, and bus transit boards in May 2010 in honor of the 15th anniversary of National Hepatitis Awareness Month and Asian Pacific Heritage Month. They showed groups of Asian-American beauty contestants, a sports team, and a family of 10 with the caption, “Which one deserves to die?”
To read entire article, click here
Read article in PDF Format
Thursday, December 30, 2010
Monday, December 13, 2010
First Ever Hep B Awareness Calendar Published

Published in AsianWeek, December 13, 2010
By Linda Ong
The first ever calendar, dedicated to raising hepatitis B awareness is launching in time for the holidays on Wednesday, December 15 at The Artists Alley in San Francisco.
The 2011 Hep B Free calendar titled “Hep B can affect any one of us…” features 13 striking Asian Americans from the Bay Area, each of whom are carriers, survivors, people with family or friends who have had Hep B, or those who are actively involved in helping to raise awareness of the disease. Both profound captions and poignant personal quotes fill the pages of each month’s spread, in addition to alarming statistics of the effects of the disease and its prevalence among the Asian Pacific Islander community.
“The calendar is outstanding because it shows the relevance of Hep B in everybody’s lives, and that it can affect anyone,” said Ronald Wong, President of Imprenta Communications Group, Inc., who volunteered his time and resources for the creative design of the calendar.
The AsianWeek Foundation and San Francisco Hep B Free produced the calendar, which was shot by L.A. – based photographer Shane Sato. Jennifer Toy provided makeup while hair was styled by Ethel O’Yang of E The Look.
“The goal of the calendar is to spread awareness of Hep B all year round,” said Angela Pang, Community Relations Manager at the AsianWeek Foundation. “When people post up the calendar on their walls, we hope that it will serve as a friendly reminder to them and their loved ones about the importance of seeing a doctor who tests for Hepatitis B, if they haven’t already.”
Also known as the “Silent Killer,” Hep B currently affects 1 in 10 Asian Pacific Islanders, compared to 1 in 1,000 of the general public, and is also one of the primary causes of liver cancer. Despite this, Hep B can be treated with an effective vaccine if an infection is detected early. Therefore, the calendar serves as a daily reminder for the public to go to their doctors to get tested.
“Because of the campaign, I asked my doctor to test me and I have encouraged so many others to do the same,” said Janet Cruz, one of the calendar models and an active volunteer in the campaign. “I am honored to be a part of this pro-active movement with such devoted members who are dedicated to eradicating this fatal disease in our community.”
Calendars cost $10 each, plus $3 for shipping and handling and can be purchased online at sfhepbfree.org/calendar/ or in-person at the AsianWeek Foundation office located at 564 Market Street, Suite 320, San Francisco (Mon. through Fri., from 9 am to 5 pm). All proceeds will go towards ending hepatitis B disease and liver cancer. For more information about the calendars, call Carrolyn Kubota at (415) 373-4003.
WHEN: Wednesday, December 15, 5-7pm
WHERE: The Artists Alley
863 Mission St.
San Francisco, CA 94122
Thursday, December 2, 2010
San Francisco Hep B Free: A Grassroots Community Coalition to Prevent Hepatitis B and Liver Cancer.
J Community Health. 2010 Dec 2. [Epub ahead of print]
Bailey MB, Shiau R, Zola J, Fernyak SE, Fang T, So SK, Chang ET.
Asian Liver Center at Stanford University, 490 S. California Ave, Suite 300, Palo Alto, CA, 94301, USA, merb00@stanford.edu.
Abstract
Chronic hepatitis B is the leading cause of liver cancer and the largest health disparity between Asian/Pacific Islanders (APIs) and the general US population. The Hep B Free model was launched to eliminate hepatitis B infection by increasing hepatitis B awareness, testing, vaccination, and treatment among APIs by building a broad, community-wide coalition. The San Francisco Hep B Free campaign is a diverse public/private collaboration unifying the API community, health care system, policy makers, businesses, and the general public in San Francisco, California. Mass-media and grassroots messaging raised citywide awareness of hepatitis B and promoted use of the existing health care system for hepatitis B screening and follow-up. Coalition partners reported semi-annually on activities, resources utilized, and system changes instituted. From 2007 to 2009, over 150 organizations contributed approximately $1,000,000 in resources to the San Francisco Hep B Free campaign. 40 educational events reached 1,100 healthcare providers, and 50% of primary care physicians pledged to screen APIs routinely for hepatitis B. Community events and fairs reached over 200,000 members of the general public. Of 3,315 API clients tested at stand-alone screening sites created by the campaign, 6.5% were found to be chronically infected and referred to follow-up care. A grassroots coalition that develops strong partnerships with diverse organizations can use existing resources to successfully increase public and healthcare provider awareness about hepatitis B among APIs, promote routine hepatitis B testing and vaccination as part of standard primary care, and ensure access to treatment for chronically infected individuals.
PMID: 21125320 [PubMed - as supplied by publisher]
Bailey MB, Shiau R, Zola J, Fernyak SE, Fang T, So SK, Chang ET.
Asian Liver Center at Stanford University, 490 S. California Ave, Suite 300, Palo Alto, CA, 94301, USA, merb00@stanford.edu.
Abstract
Chronic hepatitis B is the leading cause of liver cancer and the largest health disparity between Asian/Pacific Islanders (APIs) and the general US population. The Hep B Free model was launched to eliminate hepatitis B infection by increasing hepatitis B awareness, testing, vaccination, and treatment among APIs by building a broad, community-wide coalition. The San Francisco Hep B Free campaign is a diverse public/private collaboration unifying the API community, health care system, policy makers, businesses, and the general public in San Francisco, California. Mass-media and grassroots messaging raised citywide awareness of hepatitis B and promoted use of the existing health care system for hepatitis B screening and follow-up. Coalition partners reported semi-annually on activities, resources utilized, and system changes instituted. From 2007 to 2009, over 150 organizations contributed approximately $1,000,000 in resources to the San Francisco Hep B Free campaign. 40 educational events reached 1,100 healthcare providers, and 50% of primary care physicians pledged to screen APIs routinely for hepatitis B. Community events and fairs reached over 200,000 members of the general public. Of 3,315 API clients tested at stand-alone screening sites created by the campaign, 6.5% were found to be chronically infected and referred to follow-up care. A grassroots coalition that develops strong partnerships with diverse organizations can use existing resources to successfully increase public and healthcare provider awareness about hepatitis B among APIs, promote routine hepatitis B testing and vaccination as part of standard primary care, and ensure access to treatment for chronically infected individuals.
PMID: 21125320 [PubMed - as supplied by publisher]
Wednesday, December 1, 2010
SF Hep B Free
SF Hep B Free
Putting the Social in Theory
Wednesday, December 1, 2010
SF Hep B Free is currently going through a war of position. In this war of movement, SF Hep B Free also needs to “take the offensive more openly against the oppositionists and organise permanently the ‘impossibility’ of internal disintegration – with controls of every kind, political, administrative, etc., reinforcement of the hegominic ‘positions’ of the dominant group” (238-9). They are attempting to affect change indirectly by ensuring that various aspects of civil society can empathize and began to see what change needs to be affected. We are seeing part of Gramsci’s theory of transition occurring.
In this scenario, SF Hep B Free is attempting to change society. Here, we can view the State as a “coercive apparatus to bring the mass of the people into conformity with the specific type of production and the specific economy at a given moment” (56). Right now, Hepatitis B is not seen as national priority.
More specifically, primary providers are attempting to care for all of their patients as a whole and have less time to consider health disparities such as Hepatitis B, which might only affect a minor fraction of their patients or even none of their patients. These providers generate consent and thus, hegemony of what society is unaware of. They help generate hegemony through the whole idea that they are the people, who take care of us and have no ill-intended thoughts in their mind. They only have the intention of ensuring our well being. However, the problem in terms of Hep B awareness is that they might not know how to ensure a person’s well-being if that person might have Hepatitis B. These providers’ lack of knowledge of how to deal with a health disparity ends up leaving society to deal with the real truth of what is at stake, the rotation “of the ruling-class parties, not the foundation and organization of a new political society, and even less of a new type of civil society” (160). What is really at stake is this system, where people, who have Hepatitis B and dying from it despite the lack of resources available. The vaccine has been around since the 1960s and yet over 270 million people in the world have this disease. This cycle needs to be broken for change to be able to affect society. The best way for change to affect society is through a war of position. This war of position, “once won, is decisive definitively” (239) and as a result, change will occur. However, “the war of position demands enormous sacrifices by infinite masses of people” (239). SF Hep B Free needs to stay strong and continue to mobilize groups of support from their cause, not to just focus on Asian interest groups, but the community as a whole from churches to trade unions, and businesses.
For full blog post, click here
Putting the Social in Theory
Wednesday, December 1, 2010
SF Hep B Free is currently going through a war of position. In this war of movement, SF Hep B Free also needs to “take the offensive more openly against the oppositionists and organise permanently the ‘impossibility’ of internal disintegration – with controls of every kind, political, administrative, etc., reinforcement of the hegominic ‘positions’ of the dominant group” (238-9). They are attempting to affect change indirectly by ensuring that various aspects of civil society can empathize and began to see what change needs to be affected. We are seeing part of Gramsci’s theory of transition occurring.
In this scenario, SF Hep B Free is attempting to change society. Here, we can view the State as a “coercive apparatus to bring the mass of the people into conformity with the specific type of production and the specific economy at a given moment” (56). Right now, Hepatitis B is not seen as national priority.
More specifically, primary providers are attempting to care for all of their patients as a whole and have less time to consider health disparities such as Hepatitis B, which might only affect a minor fraction of their patients or even none of their patients. These providers generate consent and thus, hegemony of what society is unaware of. They help generate hegemony through the whole idea that they are the people, who take care of us and have no ill-intended thoughts in their mind. They only have the intention of ensuring our well being. However, the problem in terms of Hep B awareness is that they might not know how to ensure a person’s well-being if that person might have Hepatitis B. These providers’ lack of knowledge of how to deal with a health disparity ends up leaving society to deal with the real truth of what is at stake, the rotation “of the ruling-class parties, not the foundation and organization of a new political society, and even less of a new type of civil society” (160). What is really at stake is this system, where people, who have Hepatitis B and dying from it despite the lack of resources available. The vaccine has been around since the 1960s and yet over 270 million people in the world have this disease. This cycle needs to be broken for change to be able to affect society. The best way for change to affect society is through a war of position. This war of position, “once won, is decisive definitively” (239) and as a result, change will occur. However, “the war of position demands enormous sacrifices by infinite masses of people” (239). SF Hep B Free needs to stay strong and continue to mobilize groups of support from their cause, not to just focus on Asian interest groups, but the community as a whole from churches to trade unions, and businesses.
For full blog post, click here
Wednesday, September 29, 2010
HEALTHLINK: Becoming Hep B Free
This article appeared as a two-page spread in HealthLink Magazine (Fall 2010 issue, pgs. 6-7), published by Brown & Toland Physicians.
Download PDF

 Hepatitis B is linked to an increased risk of liver cancer among Asian-Americans and Pacific Islanders. Learn more about this disease and the campaign to fight it.
Hepatitis B is linked to an increased risk of liver cancer among Asian-Americans and Pacific Islanders. Learn more about this disease and the campaign to fight it.
If San Francisco becomes the first city to stamp out hepatitis B — the contagious liver infection linked to liver cancer and caused by the hepatitis B virus (HBV) — then a historic coalition of more than 50 Asian Pacific Islander (API) and healthcare organizations, including Brown & Toland Physicians, can rightfully claim to have met its goal.
Dubbed the San Francisco Hep B Free Campaign, this initiative aims to screen, vaccinate and treat all San Francisco API residents for hepatitis B by providing convenient, free or low-cost blood tests at partnering health facilities and events. Already, it has spawned similar hepatitis B campaigns across the country, from Alameda County to Philadelphia.
"As an elected official, I feel it is my responsibility to educate people about hepatitis B," says state Assemblywoman Fiona Ma, who is the campaign’s honorary chair. By encouraging the community to take swift action, she adds, "hopefully, we're saving lives."
The need to increase public awareness about hepatitis B is fully appreciated by Assemblywoman Ma, who has the virus, passed from generation to generation in her family. Once Ma understood the threat she faced as an HBV carrier (including a one in four chance of developing liver cancer), she consulted her doctor and now gets tested regularly. She urged her mother to do the same. "Last December, doctors removed a cancerous part of my mother's liver, and now she's fine," says Ma. "The message is that you have to catch hepatitis B early. My family is living proof."
Chilling Statistics, Achievable Goals
Ma's family exemplifies the virus' threat to public health: An estimated one in 10 Asians are chronically infected with hepatitis B and are four times more likely to die from liver cancer compared with the general population; San Francisco has the highest rate of liver cancer in the nation, due to its high population of Asian-Americans. The campaign’s intense efforts have been likened to the coordinated assault on AIDS and HIV, with an important exception: the imminent chance for success. "We have a safe and effective vaccine, we have good oral medications to slow or prevent liver damage, and we have decent tests to determine what someone needs," says Janet Zola of the San Francisco Department of Public Health and one of Hep B Free’s cofounders and current leads. "We just have got to get people to know it."
Getting the Public's Attention
Effective use of the media to spread the message about hepatitis B has been a vital Hep B Free strategy, owing in no small part to the pivotal involvement of one of the campaign's cofounders, Ted Fang, director of the AsianWeek Foundation, and its marketing committee, chaired by John Fisher of Brown & Toland. Print and billboard ads have been especially attention getting and feature actual members of the San Francisco API community, not professional models. "The ads have been highly visible, both locally and nationally. They get people talking about hepatitis B," says Mai-Sie Chan, M.D., a Brown & Toland internist, who’s among a group of physicians featured in the latest ads and practices in the Chinatown community. "It's a good way to participate in solving a problem that is relevant not only to the Asian Pacific Islander community but to everyone."
Download PDF
If San Francisco becomes the first city to stamp out hepatitis B — the contagious liver infection linked to liver cancer and caused by the hepatitis B virus (HBV) — then a historic coalition of more than 50 Asian Pacific Islander (API) and healthcare organizations, including Brown & Toland Physicians, can rightfully claim to have met its goal.
Dubbed the San Francisco Hep B Free Campaign, this initiative aims to screen, vaccinate and treat all San Francisco API residents for hepatitis B by providing convenient, free or low-cost blood tests at partnering health facilities and events. Already, it has spawned similar hepatitis B campaigns across the country, from Alameda County to Philadelphia.
"As an elected official, I feel it is my responsibility to educate people about hepatitis B," says state Assemblywoman Fiona Ma, who is the campaign’s honorary chair. By encouraging the community to take swift action, she adds, "hopefully, we're saving lives."
The need to increase public awareness about hepatitis B is fully appreciated by Assemblywoman Ma, who has the virus, passed from generation to generation in her family. Once Ma understood the threat she faced as an HBV carrier (including a one in four chance of developing liver cancer), she consulted her doctor and now gets tested regularly. She urged her mother to do the same. "Last December, doctors removed a cancerous part of my mother's liver, and now she's fine," says Ma. "The message is that you have to catch hepatitis B early. My family is living proof."
Chilling Statistics, Achievable Goals
Ma's family exemplifies the virus' threat to public health: An estimated one in 10 Asians are chronically infected with hepatitis B and are four times more likely to die from liver cancer compared with the general population; San Francisco has the highest rate of liver cancer in the nation, due to its high population of Asian-Americans. The campaign’s intense efforts have been likened to the coordinated assault on AIDS and HIV, with an important exception: the imminent chance for success. "We have a safe and effective vaccine, we have good oral medications to slow or prevent liver damage, and we have decent tests to determine what someone needs," says Janet Zola of the San Francisco Department of Public Health and one of Hep B Free’s cofounders and current leads. "We just have got to get people to know it."
Getting the Public's Attention
Effective use of the media to spread the message about hepatitis B has been a vital Hep B Free strategy, owing in no small part to the pivotal involvement of one of the campaign's cofounders, Ted Fang, director of the AsianWeek Foundation, and its marketing committee, chaired by John Fisher of Brown & Toland. Print and billboard ads have been especially attention getting and feature actual members of the San Francisco API community, not professional models. "The ads have been highly visible, both locally and nationally. They get people talking about hepatitis B," says Mai-Sie Chan, M.D., a Brown & Toland internist, who’s among a group of physicians featured in the latest ads and practices in the Chinatown community. "It's a good way to participate in solving a problem that is relevant not only to the Asian Pacific Islander community but to everyone."
Thursday, September 23, 2010
ANA Announces Finalists for 2010 Multicultural Excellence Awards
Advertisers Honored in Eight Categories, Including New Print Category
New York, NY - The Association of National Advertisers today announced the finalists for the 2010 Multicultural Excellence Awards. Currently in its 10th year, the awards recognize ANA member companies and other marketers for their outstanding work in producing multicultural advertising campaigns that ran between June 2009 and June 2010.
The 2010 grand prize winner in each category will be announced at a ceremony during ANA's 12th Annual Multicultural Marketing & Diversity Conference. The event will run from November 7-9 at the Fontainebleau Miami Beach in Miami, FL. For more information about the conference, including the full agenda, please visit http://www.ana.net/conference/show/id/MCC-NOV10.
This year marks the inauguration of a new category highlighting exceptional work in print advertising. In addition to print, finalists were named in seven other categories. The brand and agency finalists in each of the eight categories are listed below:
African American
• McDonald's US, Burrell Communications Group
• McDonald's US, Burrell Communications Group
• MillerCoors, commonground
Asian
• McDonald's US, IW Group, Inc.
• Metropolitan Life Insurance Company, IW Group, Inc.
• San Francisco Hep B Free Campaign, DAE
Campaign with Significant Results
• Marine Corps Recruiting Command, UniWorld Group, Inc.
• Procter & Gamble, Burrell Communications Group
• San Francisco Hep B Free Campaign, DAE
Digital Media
• Ford Motor Company, Zubi Advertising
• McDonald's US, Alma DDB
• MillerCoors, commonground
General Market Category
• 46664/Nelson Mandela Foundation, Gotham
• Procter & Gamble, Burrell Communications Group
• State Farm, Draftfcb Chicago
Hispanic
• Allstate Insurance Company, Lapiz
• McDonald's US, Alma DDB
• The Ad Council, Grupo Gallegos
Print
• California Milk Processor Board, Grupo Gallegos
• McDonald's US, IW Group, Inc.
• San Francisco Hep B Free Campaign, DAE
Radio
• Cine las Americas Film Festival, LatinWorks
• The Coca Cola Company, Ogilvy Latina
• MillerCoors, commonground
The awards are sponsored by the ANA Multicultural Marketing & Diversity Committee. Established in 1998, the committee sits at the intersection of multicultural marketing and diversity management. Its mission is to educate and inform members on key topics and issues relevant to today's multicultural marketers and diversity leaders. A portion of the proceeds collected from the awards submission fees will be used to help fund scholarships for multicultural students who plan to pursue careers in advertising and/or marketing.
# # #
About the ANA
Founded in 1910, the ANA (Association of National Advertisers) leads the marketing community by providing its members with insights, collaboration, and advocacy. ANA's membership includes 400 companies with 9,000 brands that collectively spend over $250 billion in marketing communications and advertising. The ANA strives to communicate marketing best practices, lead industry initiatives, influence industry practices, manage industry affairs, and advance, promote, and protect all advertisers and marketers. For more information, visit www.ana.net.
Press Contacts:
Lesley Neadel
CooperKatz & Co. for the ANA
lneadel@cooperkatz.com
(917) 595-3034
Luna Ross
CooperKatz & Co. for the ANA
lross@cooperkatz.com
(917) 595-3061
New York, NY - The Association of National Advertisers today announced the finalists for the 2010 Multicultural Excellence Awards. Currently in its 10th year, the awards recognize ANA member companies and other marketers for their outstanding work in producing multicultural advertising campaigns that ran between June 2009 and June 2010.
The 2010 grand prize winner in each category will be announced at a ceremony during ANA's 12th Annual Multicultural Marketing & Diversity Conference. The event will run from November 7-9 at the Fontainebleau Miami Beach in Miami, FL. For more information about the conference, including the full agenda, please visit http://www.ana.net/conference/show/id/MCC-NOV10.
This year marks the inauguration of a new category highlighting exceptional work in print advertising. In addition to print, finalists were named in seven other categories. The brand and agency finalists in each of the eight categories are listed below:
African American
• McDonald's US, Burrell Communications Group
• McDonald's US, Burrell Communications Group
• MillerCoors, commonground
Asian
• McDonald's US, IW Group, Inc.
• Metropolitan Life Insurance Company, IW Group, Inc.
• San Francisco Hep B Free Campaign, DAE
Campaign with Significant Results
• Marine Corps Recruiting Command, UniWorld Group, Inc.
• Procter & Gamble, Burrell Communications Group
• San Francisco Hep B Free Campaign, DAE
Digital Media
• Ford Motor Company, Zubi Advertising
• McDonald's US, Alma DDB
• MillerCoors, commonground
General Market Category
• 46664/Nelson Mandela Foundation, Gotham
• Procter & Gamble, Burrell Communications Group
• State Farm, Draftfcb Chicago
Hispanic
• Allstate Insurance Company, Lapiz
• McDonald's US, Alma DDB
• The Ad Council, Grupo Gallegos
• California Milk Processor Board, Grupo Gallegos
• McDonald's US, IW Group, Inc.
• San Francisco Hep B Free Campaign, DAE
Radio
• Cine las Americas Film Festival, LatinWorks
• The Coca Cola Company, Ogilvy Latina
• MillerCoors, commonground
The awards are sponsored by the ANA Multicultural Marketing & Diversity Committee. Established in 1998, the committee sits at the intersection of multicultural marketing and diversity management. Its mission is to educate and inform members on key topics and issues relevant to today's multicultural marketers and diversity leaders. A portion of the proceeds collected from the awards submission fees will be used to help fund scholarships for multicultural students who plan to pursue careers in advertising and/or marketing.
# # #
About the ANA
Founded in 1910, the ANA (Association of National Advertisers) leads the marketing community by providing its members with insights, collaboration, and advocacy. ANA's membership includes 400 companies with 9,000 brands that collectively spend over $250 billion in marketing communications and advertising. The ANA strives to communicate marketing best practices, lead industry initiatives, influence industry practices, manage industry affairs, and advance, promote, and protect all advertisers and marketers. For more information, visit www.ana.net.
Press Contacts:
Lesley Neadel
CooperKatz & Co. for the ANA
lneadel@cooperkatz.com
(917) 595-3034
Luna Ross
CooperKatz & Co. for the ANA
lross@cooperkatz.com
(917) 595-3061
Wednesday, September 22, 2010
National Hep B Community Gathers in San Francisco To Honor Nobel Laureate Dr. Baruch Blumberg and SF Hep B Free
By Grace Niwa - AsianWeek.com
 Left to right:
Left to right:
Meredith Bergin Bailey, Asian Liver Center, Dr. Stuart Fong, Chinese Hospital, Dr. Baruch Blumberg, Dr. Joseph Woo, Chinese Hospital, Ted Fang, AsianWeek Foundation & SF Hep B Free, Janet Zola, SF Department of Public Health & SF Hep B Free, John Fisher, Brown and Toland Physicians Group.
San Francisco – Nobel Laureate Dr. Baruch Blumberg, discoverer of the Hepatitis B virus and developer of its vaccine was honored at San Francisco’s Hepatitis B Free Coast to Coast Awards Gala on September 16 at The Regency Center. Co-host Chinese Hospital presented its 37th Annual Award to Dr. Blumberg for his contribution to improving the health of Asians. Dr. Blumberg was also presented with the 3rd Annual Hep B Free Super Hero Award which includes a blue cape with the “B Superhero” emblem emblazoned on the back. The night’s event was presented by SF Hep B Free and Chinese Hospital, and produced by the AsianWeek Foundation.
“The means are available to prevent and treat hepatitis B,” said Blumberg. “These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are educated about the virus and take part in the program of vaccination, detection, and treatment. The Chinese Hospital, San Francisco Hep B Free Campaign, Hepatitis B Foundation in Philadelphia and other Hep B Free initiatives across the nation are making the public aware of the problem and leading the efforts to solve it.”
Emceed by Hepatitis B spokespersons, California State Assemblywoman Fiona Ma and ABC7 Anchor/Reporter Alan Wang, over 600 people attended. Special guests included Joan Block, Executive Director, Hepatitis B Foundation, Dr. Moon Chen, UC Davis, Asian American Network for Cancer Awareness, Research and Training, Jeff Cabellero, Association of Asian Pacific Community Health Organizations, Dr. Mitch Katz, Chief Public Health Officer for San Francisco, Dr. Ed Chow, Health Commissioner, Mark Leno, State Senator, David Chiu, President, SF Board of Supervisors, Carmen Chu, Supervisor Bevan Dufty, Supervisor and James Fang, President, BART Board.
Hep B Free Philadelphia is a public awareness and education campaign – based on the enormously successful San Francisco Hep B Free campaign,” said Joan Block, Executive Director & Co-Founder, Hepatitis B Foundation. “We felt the time was right in creating this initiative. We want to feel a part of a larger movement for change because together, we can do more to help people and save lives.”
Deaths from liver cancer are rising faster than any other cancer in America. San Francisco’s Hep B Free public health project is leading the country as a healthcare reform model. A unique collaboration of over 50 private and public organizations, its goal is to turn San Francisco into the first city in America to be free of hepatitis B transmission, which is responsible for up to 80% of all liver cancer. Their innovative campaign also addresses the disease as the greatest health disparity for Asian Pacific Americans in the nation, and in the world. Based on the enormously successful SF Hep B Free campaign, other counties and cities are starting to replicate its model. They include Los Angeles, Orange County, Santa Clara, Alameda, Long Beach, San Mateo, Philadelphia, and Washington, DC.
SF Hep B Free is the country’s first initiative to utilize healthcare reform principles, including electronic medical records and quality assurance measures, for addressing a leading health disparity and a deadly chronic disease. The program has received national coverage in the New York Times, PBS News Hour, NPR’s Morning Edition, San Francisco Chronicle and others.
Left to right:Meredith Bergin Bailey, Asian Liver Center, Dr. Stuart Fong, Chinese Hospital, Dr. Baruch Blumberg, Dr. Joseph Woo, Chinese Hospital, Ted Fang, AsianWeek Foundation & SF Hep B Free, Janet Zola, SF Department of Public Health & SF Hep B Free, John Fisher, Brown and Toland Physicians Group.
San Francisco – Nobel Laureate Dr. Baruch Blumberg, discoverer of the Hepatitis B virus and developer of its vaccine was honored at San Francisco’s Hepatitis B Free Coast to Coast Awards Gala on September 16 at The Regency Center. Co-host Chinese Hospital presented its 37th Annual Award to Dr. Blumberg for his contribution to improving the health of Asians. Dr. Blumberg was also presented with the 3rd Annual Hep B Free Super Hero Award which includes a blue cape with the “B Superhero” emblem emblazoned on the back. The night’s event was presented by SF Hep B Free and Chinese Hospital, and produced by the AsianWeek Foundation.
“The means are available to prevent and treat hepatitis B,” said Blumberg. “These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are educated about the virus and take part in the program of vaccination, detection, and treatment. The Chinese Hospital, San Francisco Hep B Free Campaign, Hepatitis B Foundation in Philadelphia and other Hep B Free initiatives across the nation are making the public aware of the problem and leading the efforts to solve it.”
Emceed by Hepatitis B spokespersons, California State Assemblywoman Fiona Ma and ABC7 Anchor/Reporter Alan Wang, over 600 people attended. Special guests included Joan Block, Executive Director, Hepatitis B Foundation, Dr. Moon Chen, UC Davis, Asian American Network for Cancer Awareness, Research and Training, Jeff Cabellero, Association of Asian Pacific Community Health Organizations, Dr. Mitch Katz, Chief Public Health Officer for San Francisco, Dr. Ed Chow, Health Commissioner, Mark Leno, State Senator, David Chiu, President, SF Board of Supervisors, Carmen Chu, Supervisor Bevan Dufty, Supervisor and James Fang, President, BART Board.
Hep B Free Philadelphia is a public awareness and education campaign – based on the enormously successful San Francisco Hep B Free campaign,” said Joan Block, Executive Director & Co-Founder, Hepatitis B Foundation. “We felt the time was right in creating this initiative. We want to feel a part of a larger movement for change because together, we can do more to help people and save lives.”
Deaths from liver cancer are rising faster than any other cancer in America. San Francisco’s Hep B Free public health project is leading the country as a healthcare reform model. A unique collaboration of over 50 private and public organizations, its goal is to turn San Francisco into the first city in America to be free of hepatitis B transmission, which is responsible for up to 80% of all liver cancer. Their innovative campaign also addresses the disease as the greatest health disparity for Asian Pacific Americans in the nation, and in the world. Based on the enormously successful SF Hep B Free campaign, other counties and cities are starting to replicate its model. They include Los Angeles, Orange County, Santa Clara, Alameda, Long Beach, San Mateo, Philadelphia, and Washington, DC.
SF Hep B Free is the country’s first initiative to utilize healthcare reform principles, including electronic medical records and quality assurance measures, for addressing a leading health disparity and a deadly chronic disease. The program has received national coverage in the New York Times, PBS News Hour, NPR’s Morning Edition, San Francisco Chronicle and others.
Monday, September 20, 2010
Event Photos - Week of Sept. 13, 2010
9-15-10 Hep B Panel Discussion with Asia Society
Click here to see photos
9-16-10 CME Luncheon & news conference @ Chinese Hospital Honors Dr Baruch Blumberg
Click here to see photos
9-16-10 Hep B Free Coast to Coast Gala Honoring Dr Baruch Blumberg
Click here to see photos
Click here to see photos
9-16-10 CME Luncheon & news conference @ Chinese Hospital Honors Dr Baruch Blumberg
Click here to see photos
9-16-10 Hep B Free Coast to Coast Gala Honoring Dr Baruch Blumberg
Click here to see photos
Sunday, September 19, 2010
SF Examiner: Public health specialist works to raise hepatitis B awareness
By: Brent Begin | Examiner Staff Writer

Janet Zola, the health promotion specialist at the Department of Public Health and co-creator of "SF Hep B Free," was part of a week of events to raise awareness about hepatitis B in the Asian and Pacific Islander population (API).
What is Hep B Free? It’s a broad spectrum coalition of people in health care, the Asian-American community, businesses and nonprofits all coming together to stop the spread of hepatitis B and liver cancer.
Why the Asian-American community? In the API population there is a 10 percent infection rate. This is chronic, as it is less than 1 percent in the general population. It is one of the greatest health disparities we’ve seen.
How do you get the disease? The disease is generally passed on at birth. Over half the people infected are unaware of it. When you become affected at a very early age there are no symptoms. Only simple blood tests can tell you.
Can you get it any other way? It’s also a blood borne disease that can be transmitted sexually or through needles. Hepatitis B is about 100 times more infectious than HIV.
What’s the problem with fighting this disease? The great thing is we have all the tools to prevent and fight this disease. The problem is the lack of knowledge, lack of awareness and lack of funding support.
Janet Zola, the health promotion specialist at the Department of Public Health and co-creator of "SF Hep B Free," was part of a week of events to raise awareness about hepatitis B in the Asian and Pacific Islander population (API).
What is Hep B Free? It’s a broad spectrum coalition of people in health care, the Asian-American community, businesses and nonprofits all coming together to stop the spread of hepatitis B and liver cancer.
Why the Asian-American community? In the API population there is a 10 percent infection rate. This is chronic, as it is less than 1 percent in the general population. It is one of the greatest health disparities we’ve seen.
How do you get the disease? The disease is generally passed on at birth. Over half the people infected are unaware of it. When you become affected at a very early age there are no symptoms. Only simple blood tests can tell you.
Can you get it any other way? It’s also a blood borne disease that can be transmitted sexually or through needles. Hepatitis B is about 100 times more infectious than HIV.
What’s the problem with fighting this disease? The great thing is we have all the tools to prevent and fight this disease. The problem is the lack of knowledge, lack of awareness and lack of funding support.
Friday, September 17, 2010
Business Times: S.F.'s hepatitis B campaign now a model
By Ron Leuty, Reporter | Read full article
San Francisco's Hep B Free campaign, aimed at eradicating one of the Asian-American community’s biggest killers, is being copied nationwide.

Ted Fang, director of the AsianWeek Foundation and a driver behind San Francisco's campaign, said as many as a dozen communities, including Philadelphia, "are trying replicate the model here in San Francisco."
Speaking at an event Wednesday that featured Baruch Blumberg, the Nobel Prize-winning discoverer of the hepatitis B virus and vaccine, Fang said Hep B Free is helping to erase the stigma of a disease that left untreated can lead to deadly liver cancer.
San Francisco, not coincidentally, has the highest liver cancer rate in the United States, according to the group.
Hep B Free brought together city government, private health care providers and businesses. Key to the campaign has been ads on buses and at Muni shelters that show different groups of 10 Asian-Americans and a tagline, "Which one deserves to die?"
That refers to the fact that one in 10 in the Asian-American community is chronically infected with the disease.
(In the attached video, Fang talks about how Hep B Free has tapped the unique characteristics of the Asian-American community — including 90 percent coverage by health insurance, according to Fang — to get San Francisco hospitals involved.)
Hep B Free now is asking every primary care doctor in San Francisco to sign a pledge to test at-risk patients for hep B. Sixty percent have signed up, Fang said, including all physicians at 54-bed Chinese Hospital, North East Medical Services in Chinatown and Kaiser Permanente.
"This is not just an Asian problem," said Samuel So. director of the Asian Liver Center at Stanford University. "This is a community problem. This is an American problem."
Email Ron Leuty at rleuty@bizjournals.com
San Francisco's Hep B Free campaign, aimed at eradicating one of the Asian-American community’s biggest killers, is being copied nationwide.
A Hep B Free campaign ad in a San Francisco bus.
Speaking at an event Wednesday that featured Baruch Blumberg, the Nobel Prize-winning discoverer of the hepatitis B virus and vaccine, Fang said Hep B Free is helping to erase the stigma of a disease that left untreated can lead to deadly liver cancer.
San Francisco, not coincidentally, has the highest liver cancer rate in the United States, according to the group.
Hep B Free brought together city government, private health care providers and businesses. Key to the campaign has been ads on buses and at Muni shelters that show different groups of 10 Asian-Americans and a tagline, "Which one deserves to die?"
That refers to the fact that one in 10 in the Asian-American community is chronically infected with the disease.
(In the attached video, Fang talks about how Hep B Free has tapped the unique characteristics of the Asian-American community — including 90 percent coverage by health insurance, according to Fang — to get San Francisco hospitals involved.)
Hep B Free now is asking every primary care doctor in San Francisco to sign a pledge to test at-risk patients for hep B. Sixty percent have signed up, Fang said, including all physicians at 54-bed Chinese Hospital, North East Medical Services in Chinatown and Kaiser Permanente.
"This is not just an Asian problem," said Samuel So. director of the Asian Liver Center at Stanford University. "This is a community problem. This is an American problem."
Email Ron Leuty at rleuty@bizjournals.com
Hepatitis B Prevention Program Gaining Traction in San Francisco
Author: Steven Fox | Download PDF | See online version
 September 17, 2010 (San Francisco, California) — A unique community-based program aimed at preventing hepatitis B in the high-risk Asian population is effectively combining provocative advertising with electronic medical records (EMRs) to maximize its success.
September 17, 2010 (San Francisco, California) — A unique community-based program aimed at preventing hepatitis B in the high-risk Asian population is effectively combining provocative advertising with electronic medical records (EMRs) to maximize its success.
The program, known as San Francisco Hep B Free, is a collaborative effort of more than 50 private and public organizations that was launched 3 years ago. It sponsors numerous screening clinics, works with hospitals and primary care physicians to make screening a part of routine care, and tracks the treatment of people who are already infected with the virus.
The program works with hospitals to get pledges from physicians to routinely screen their patients for the presence of hepatitis B virus. So far, nearly half the primary care physicians in the city have signed on to the program. They have agreed to assess all at-risk patients according to Centers for Disease Control and Prevention guidelines. Three facilities — Kaiser Permanente San Francisco, the Chinese Hospital, and Northeast Medical Services — have achieved 100% physician buy-in to the program.
Challenges remain, however. "Changing practice patterns of primary care physicians is the most difficult aspect of what we do," said Ted Fang, an Asian community organizer who helped get Hep B Free started and who now works with scores of other community organizers and healthcare professionals to steer the program. "That's because of all the responsibilities doctors already have and the limited time they have to spend with each patient."
The need for attention to hepatitis B is hardly at issue, Mr. Fang noted. The disease is the prime causative factor in about 80% of liver cancers, according to World Health Organization figures, and San Francisco has the highest rate of liver cancer in the nation — about 14 cases per 100,000, compared with 9.5 cases per 100,000 in the rest of the country.
Hep B Free operates 7 stand-alone screening clinics and hosts community screening fairs that are aimed at reaching uninsured and underinsured patients.
A print and television advertising campaign that made its debut in May 2010 has helped bolster awareness of the Hep B Free program — but it has also raised a few eyebrows. Each ad features a different group of Asians — beauty queens, athletes, office workers, physicians — with the caption: "Which one deserves to die?"
Mr. Fang concedes it's a strong approach, but said the ads have produced the desired result: getting people talking about the disease, both among themselves and with their doctors. The print ads are being published in Chinese, Vietnamese, and Korean, and in English because one of the target groups is English-speaking physicians who might not be aware of the prevalence of the disease in the Asian community.
EMRs play a role in making the Hep B Free program a success. They are put to use in several phases of the program:
* For people who don't know their hepatitis B status, EMRs can be flagged to ensure that they are properly screened.
* For people being vaccinated, EMRs help track compliance to the full vaccination series (3 injections administered over 6 months).
* For people chronically infected, EMRs can generate reminders to contact patients for annual or semiannual monitoring.
"There is no way we can improve healthcare outcomes unless we can evaluate the effectiveness of current medical services," said Mr. Fang. "EMRs not only remind doctors to carry out important procedures, they also help evaluate which methods of prevention work best and which we need to improve."
Another major partner in administering the Hep B Free program is the San Francisco Department of Public Health (DPH). Janet Zola, MPH, is disease prevention and health promotion specialist there, and was a key player in developing the Hep B Free program.
That was just the start. According to Ms. Zola, "the DPH allows me to use a large percentage of my time to run the campaign, coordinate activities, and do strategic planning."
She added that she's learned several important lessons from running the program. "Resources can be leveraged without waiting for an infusion of large amounts of money," she explained. Getting cooperation from local hospitals is important, but community support has been essential to the success of the program so far, she asserted. "Volunteerism is alive and well," she added. "This is more than an Asian problem. It is an American problem."
The success of San Francisco Hep B Free hasn't gone unnoticed. Other California cities, plus Philadelphia, Pennsylvania, and Washington, DC, are working to replicate the program.
That progress is good news to Baruch Blumberg, MD, PhD, who has a special interest in hepatitis B. He received the Nobel Prize for Medicine in 1976 for his discovery of the hepatitis B virus, and later developed the first effective vaccine for the disease. The vaccine became available in the early 1980s.
Dr. Blumberg was recently honored at a dinner reception jointly sponsored by the Hep B Free program and the Chinese Hospital.
Noting that vaccines and effective treatments for hepatitis B are now potentially available worldwide, Dr. Blumberg told Medscape Medical News that the key to reducing the toll of the disease lies in continuing to increase awareness.
"These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are aware of the problem and take part in programs that include vaccination, detection, and treatment," said Dr. Blumberg.
The program, known as San Francisco Hep B Free, is a collaborative effort of more than 50 private and public organizations that was launched 3 years ago. It sponsors numerous screening clinics, works with hospitals and primary care physicians to make screening a part of routine care, and tracks the treatment of people who are already infected with the virus.
The program works with hospitals to get pledges from physicians to routinely screen their patients for the presence of hepatitis B virus. So far, nearly half the primary care physicians in the city have signed on to the program. They have agreed to assess all at-risk patients according to Centers for Disease Control and Prevention guidelines. Three facilities — Kaiser Permanente San Francisco, the Chinese Hospital, and Northeast Medical Services — have achieved 100% physician buy-in to the program.
Challenges remain, however. "Changing practice patterns of primary care physicians is the most difficult aspect of what we do," said Ted Fang, an Asian community organizer who helped get Hep B Free started and who now works with scores of other community organizers and healthcare professionals to steer the program. "That's because of all the responsibilities doctors already have and the limited time they have to spend with each patient."
The need for attention to hepatitis B is hardly at issue, Mr. Fang noted. The disease is the prime causative factor in about 80% of liver cancers, according to World Health Organization figures, and San Francisco has the highest rate of liver cancer in the nation — about 14 cases per 100,000, compared with 9.5 cases per 100,000 in the rest of the country.
Hep B Free operates 7 stand-alone screening clinics and hosts community screening fairs that are aimed at reaching uninsured and underinsured patients.
A print and television advertising campaign that made its debut in May 2010 has helped bolster awareness of the Hep B Free program — but it has also raised a few eyebrows. Each ad features a different group of Asians — beauty queens, athletes, office workers, physicians — with the caption: "Which one deserves to die?"
Mr. Fang concedes it's a strong approach, but said the ads have produced the desired result: getting people talking about the disease, both among themselves and with their doctors. The print ads are being published in Chinese, Vietnamese, and Korean, and in English because one of the target groups is English-speaking physicians who might not be aware of the prevalence of the disease in the Asian community.
EMRs play a role in making the Hep B Free program a success. They are put to use in several phases of the program:
* For people who don't know their hepatitis B status, EMRs can be flagged to ensure that they are properly screened.
* For people being vaccinated, EMRs help track compliance to the full vaccination series (3 injections administered over 6 months).
* For people chronically infected, EMRs can generate reminders to contact patients for annual or semiannual monitoring.
"There is no way we can improve healthcare outcomes unless we can evaluate the effectiveness of current medical services," said Mr. Fang. "EMRs not only remind doctors to carry out important procedures, they also help evaluate which methods of prevention work best and which we need to improve."
Another major partner in administering the Hep B Free program is the San Francisco Department of Public Health (DPH). Janet Zola, MPH, is disease prevention and health promotion specialist there, and was a key player in developing the Hep B Free program.
That was just the start. According to Ms. Zola, "the DPH allows me to use a large percentage of my time to run the campaign, coordinate activities, and do strategic planning."
She added that she's learned several important lessons from running the program. "Resources can be leveraged without waiting for an infusion of large amounts of money," she explained. Getting cooperation from local hospitals is important, but community support has been essential to the success of the program so far, she asserted. "Volunteerism is alive and well," she added. "This is more than an Asian problem. It is an American problem."
The success of San Francisco Hep B Free hasn't gone unnoticed. Other California cities, plus Philadelphia, Pennsylvania, and Washington, DC, are working to replicate the program.
That progress is good news to Baruch Blumberg, MD, PhD, who has a special interest in hepatitis B. He received the Nobel Prize for Medicine in 1976 for his discovery of the hepatitis B virus, and later developed the first effective vaccine for the disease. The vaccine became available in the early 1980s.
Dr. Blumberg was recently honored at a dinner reception jointly sponsored by the Hep B Free program and the Chinese Hospital.
Noting that vaccines and effective treatments for hepatitis B are now potentially available worldwide, Dr. Blumberg told Medscape Medical News that the key to reducing the toll of the disease lies in continuing to increase awareness.
"These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are aware of the problem and take part in programs that include vaccination, detection, and treatment," said Dr. Blumberg.
San Francisco's "Hep B Free" Campaign a Model For The Rest of the Country
Reappropriate.com article
I’ve heard a lot lately about San Francisco’s Hep B Free campaign, a public campaign to increase hepatitis B awareness and vaccination in the Bay Area. According to Hep B Free’s website, Hepatitis B — which results from infection by the HBV virus – causes liver cancer in 80% of diagnosed patients. Further, the bloodborne HBV virus can survive for more than 7 days outside of the body and is 100 times more infectious than HIV. Sadly, HBV infections are frequently missed by primary care physicians even though diagnosis only requires a simple blood test.
Currently, 1.25 million Americans are infected with HBV, of which roughly half are Asian American. In fact, HBV is one of the leading causes of death for the Asian American community; 1 in 10 Asian Americans are currently infected with Hepatitis B.
In a talk to the 2nd annual Asian American Health Conference, Dr. Francisco Sy of the NIH noted some of the cultural and linguistic barriers that appear to influence the high HBV infection rates amongst Asian Americans:
--
Decrying that too many health academics do too much “helicopter” research in minority communities — i.e., go in and out to study the population in the short term without really getting to know them — Dr. Sy argued that “community is so important and we need to be treated as partners [in health studies] and not guinea pigs.”
Dr. Sy also contended that the stereotype which characterizes Asian Americans as the “model minority” has contributed to the dearth on health data for the group, a detriment for the community because data is what gets institutions like the NIH to give money to do further studies or finance programs.
“If there is no data,” said Dr. Sy, “there is no funding and communities suffer because Asian Americans are considered Ômodel minorities’ then people think they don’t have any [health] problems.”
The reality indeed is far from such assumptions. According to Dr. Sy, 21% of Asian Americans are uninsured and 12.5% live below the poverty line. Many also have language barriers which, along with the lack of financial resources, keep them form navigating America’s convoluted healthcare system.
Dr. Sy also mentioned that the group’s social and cultural practices — like putting the family over the self, holding a fatalistic view of illness or subscribing to more “traditional” types of healing (for Filipinos this include prayer and religious healing) and keeping topics like domestic violence and sexual orientation taboo have acted as barriers for a healthier Asian American community.
--
On the West Coast, several campaigns have worked tirelessly within the community to try and break down some of these barriers. Ted Fang, of Asian Week, who is one of the vocal leaders of San Francisco Hep B Free discussed (in the video above) how the high insurance rates of Asian Americans — some 90% of Asian Americans have health insurance — means that it’s not just about improving access to healthcare. Instead, specifically tailored awareness campaigns aimed at both patients and primary care physicians, are needed to break down the cultural stigmas around Hepatitis B.
Not surprisingly, the strategy of actually collecting community-specific data about a disease that disproportionately affects said community actually works. Fang reports in the article that nearly two-thirds of San Francisco doctors have pledged to test at-risk patients for Hepatitis B, and the Hep B Free campaign in the Bay Area is now being considered for adoption in other cities around the country.
It’s great to see recognition for those community leaders who are in the trenches, working on a non-glamorous, but nonetheless important, problem like Hepatitis B. Furthermore, their efforts speak to the critical necessity for more large race-specific, epidemiological studies, so that we can start more dialogues on stigmatized health issues and begin to identify new ways to help save lives within the APIA community.
I’ve heard a lot lately about San Francisco’s Hep B Free campaign, a public campaign to increase hepatitis B awareness and vaccination in the Bay Area. According to Hep B Free’s website, Hepatitis B — which results from infection by the HBV virus – causes liver cancer in 80% of diagnosed patients. Further, the bloodborne HBV virus can survive for more than 7 days outside of the body and is 100 times more infectious than HIV. Sadly, HBV infections are frequently missed by primary care physicians even though diagnosis only requires a simple blood test.
Currently, 1.25 million Americans are infected with HBV, of which roughly half are Asian American. In fact, HBV is one of the leading causes of death for the Asian American community; 1 in 10 Asian Americans are currently infected with Hepatitis B.
In a talk to the 2nd annual Asian American Health Conference, Dr. Francisco Sy of the NIH noted some of the cultural and linguistic barriers that appear to influence the high HBV infection rates amongst Asian Americans:
--
Decrying that too many health academics do too much “helicopter” research in minority communities — i.e., go in and out to study the population in the short term without really getting to know them — Dr. Sy argued that “community is so important and we need to be treated as partners [in health studies] and not guinea pigs.”
Dr. Sy also contended that the stereotype which characterizes Asian Americans as the “model minority” has contributed to the dearth on health data for the group, a detriment for the community because data is what gets institutions like the NIH to give money to do further studies or finance programs.
“If there is no data,” said Dr. Sy, “there is no funding and communities suffer because Asian Americans are considered Ômodel minorities’ then people think they don’t have any [health] problems.”
The reality indeed is far from such assumptions. According to Dr. Sy, 21% of Asian Americans are uninsured and 12.5% live below the poverty line. Many also have language barriers which, along with the lack of financial resources, keep them form navigating America’s convoluted healthcare system.
Dr. Sy also mentioned that the group’s social and cultural practices — like putting the family over the self, holding a fatalistic view of illness or subscribing to more “traditional” types of healing (for Filipinos this include prayer and religious healing) and keeping topics like domestic violence and sexual orientation taboo have acted as barriers for a healthier Asian American community.
--
On the West Coast, several campaigns have worked tirelessly within the community to try and break down some of these barriers. Ted Fang, of Asian Week, who is one of the vocal leaders of San Francisco Hep B Free discussed (in the video above) how the high insurance rates of Asian Americans — some 90% of Asian Americans have health insurance — means that it’s not just about improving access to healthcare. Instead, specifically tailored awareness campaigns aimed at both patients and primary care physicians, are needed to break down the cultural stigmas around Hepatitis B.
Not surprisingly, the strategy of actually collecting community-specific data about a disease that disproportionately affects said community actually works. Fang reports in the article that nearly two-thirds of San Francisco doctors have pledged to test at-risk patients for Hepatitis B, and the Hep B Free campaign in the Bay Area is now being considered for adoption in other cities around the country.
It’s great to see recognition for those community leaders who are in the trenches, working on a non-glamorous, but nonetheless important, problem like Hepatitis B. Furthermore, their efforts speak to the critical necessity for more large race-specific, epidemiological studies, so that we can start more dialogues on stigmatized health issues and begin to identify new ways to help save lives within the APIA community.
Wednesday, September 8, 2010
Controversial Ad Campaign Creates Headlines Nationwide
By Angela Pang | Read full article
SAN FRANCISCO – “Which one deserves to die?” – the controversial message featuring ten smiling Asian American physicians, beauty queens, basketball players, family members, and office workers has generated coast-to-coast buzz and headlines for the Hep B free movement.

Prominent nationwide print, television, and radio news organizations have featured the provocative ad campaign which brings the issue of death, caused by liver cancer, to the forefront, including the New York Times, San Francisco Chronicle, National Public Radio, and PBS News Hour to and local and ethnic Bay Area media.
Sunny Teo, Executive Creative Director of DAE Advertising and the brainchild behind the campaign, says it was vital to have such a shocking message to alert the public that 1 in 10 Asian and Pacific Islanders is chronically infected with hepatitis B compared to 1 in 1,000 for non-Asians.
The campaign appeared in local ethnic and mainstream newspapers, billboards, and bus transit boards in May 2010 in honor of 15th Anniversary of National Hepatitis Awareness Month and Asian Pacific Heritage Month. The campaign addressed the biggest reason for the Hep B epidemic: general lack of awareness about the disease especially among the Asian community who considers discussing illness and death a taboo.

“We felt in order to have impact, our communication needed to directly address the issue of death with a sense of urgency that involved families and social circles,” says Teo, whose company offered their serivces pro bono to the SF Hep B Free Campaign. “Anything softer would have resulted in an ad campaign with messages that nobody paid attention to or cared about.”
The intended provocative nature of the campaign even caused concern among some of the volunteer community models in the photo shoots.
“For months, there were concerns and debates, internally at the agency and within the Sf Hep B Free steering committee, about repercussions. There were fears of negative reactions [from the community] up to the eve of the launch,” recalls Teo. “But we believe the true message behind this came through—that everyone deserves to live, no one deserves to die.”
Teo believes the reasons the ad campaign has successfully resonated with the public is because of a combination of factors – the hard to ignore 1 in 10 statistics, the possibility of deatlh – one of life’s most fundamental subjects, and the participatory approach of the ads.
Grace Niwa, principal of Niwa Public Relations, suggests the ad campaign was such a hit because the models were “real people” from the Bay Area’s Asian American community.
“This brought the message close to home, since you could relate to the photo of someone that resembles a friend or family member,” says Niwa. “This also reminds the general public that anyone can be affected by Hep B and we should all work together to end Hep B and liver cancer.”
Niwa has been with SF Hep B Free since its inception in 2007 and says it has been very exciting to see Hep B Free evolve and become a national movement for Asian Pacific America. Her remarks were underlined by Ted Fang of the AsianWeek Foundation, a co-founder and Steering Committee member for SF Hep B Free. AsianWeek Foundation’s mission is to develop and promote the Asian American community.
“This is the first major market advertising campaign to feature all Asian American models, and Hep B Free is the largest organized social campaign ever for the Asian Pacific America,” said Fang. “Those are both milestones in the evolution of our community.”
Nobel Laureate Dr. Baruch Blumberg who discovered the Hepatitis B Virus and developed the Hepatitis Vaccine will be honored by the Chinese Hospital and San Francisco’s Hepatitis B community. The honor will take place at the Hep B Free Coast to Coast dinner on September 16 at the Regency Grand Ballroom. For ticket or sponsorship information, please go to sfhepbfree.org/gala/.
SAN FRANCISCO – “Which one deserves to die?” – the controversial message featuring ten smiling Asian American physicians, beauty queens, basketball players, family members, and office workers has generated coast-to-coast buzz and headlines for the Hep B free movement.

Ten Bay Area physicians.
Prominent nationwide print, television, and radio news organizations have featured the provocative ad campaign which brings the issue of death, caused by liver cancer, to the forefront, including the New York Times, San Francisco Chronicle, National Public Radio, and PBS News Hour to and local and ethnic Bay Area media.
Sunny Teo, Executive Creative Director of DAE Advertising and the brainchild behind the campaign, says it was vital to have such a shocking message to alert the public that 1 in 10 Asian and Pacific Islanders is chronically infected with hepatitis B compared to 1 in 1,000 for non-Asians.
The campaign appeared in local ethnic and mainstream newspapers, billboards, and bus transit boards in May 2010 in honor of 15th Anniversary of National Hepatitis Awareness Month and Asian Pacific Heritage Month. The campaign addressed the biggest reason for the Hep B epidemic: general lack of awareness about the disease especially among the Asian community who considers discussing illness and death a taboo.

A Chinese version of the ad.
“We felt in order to have impact, our communication needed to directly address the issue of death with a sense of urgency that involved families and social circles,” says Teo, whose company offered their serivces pro bono to the SF Hep B Free Campaign. “Anything softer would have resulted in an ad campaign with messages that nobody paid attention to or cared about.”
The intended provocative nature of the campaign even caused concern among some of the volunteer community models in the photo shoots.
“For months, there were concerns and debates, internally at the agency and within the Sf Hep B Free steering committee, about repercussions. There were fears of negative reactions [from the community] up to the eve of the launch,” recalls Teo. “But we believe the true message behind this came through—that everyone deserves to live, no one deserves to die.”
Teo believes the reasons the ad campaign has successfully resonated with the public is because of a combination of factors – the hard to ignore 1 in 10 statistics, the possibility of deatlh – one of life’s most fundamental subjects, and the participatory approach of the ads.

- Tagalog version of the ad

Grace Niwa, principal of Niwa Public Relations, suggests the ad campaign was such a hit because the models were “real people” from the Bay Area’s Asian American community.
“This brought the message close to home, since you could relate to the photo of someone that resembles a friend or family member,” says Niwa. “This also reminds the general public that anyone can be affected by Hep B and we should all work together to end Hep B and liver cancer.”
Niwa has been with SF Hep B Free since its inception in 2007 and says it has been very exciting to see Hep B Free evolve and become a national movement for Asian Pacific America. Her remarks were underlined by Ted Fang of the AsianWeek Foundation, a co-founder and Steering Committee member for SF Hep B Free. AsianWeek Foundation’s mission is to develop and promote the Asian American community.
“This is the first major market advertising campaign to feature all Asian American models, and Hep B Free is the largest organized social campaign ever for the Asian Pacific America,” said Fang. “Those are both milestones in the evolution of our community.”
Nobel Laureate Dr. Baruch Blumberg who discovered the Hepatitis B Virus and developed the Hepatitis Vaccine will be honored by the Chinese Hospital and San Francisco’s Hepatitis B community. The honor will take place at the Hep B Free Coast to Coast dinner on September 16 at the Regency Grand Ballroom. For ticket or sponsorship information, please go to sfhepbfree.org/gala/.
Tuesday, September 7, 2010
Fighting Hep B Panel Discussion
By Angela Pang – September 7, 2010 (AsianWeek.com)
 Ten percent of Asian & Pacific Islanders in the United States have chronic hepatitis B. With its sizable API population, nowhere is the HBV epidemic more pronounced and visible than in the Bay Area, which has the highest rate of liver cancer in the nation.
Ten percent of Asian & Pacific Islanders in the United States have chronic hepatitis B. With its sizable API population, nowhere is the HBV epidemic more pronounced and visible than in the Bay Area, which has the highest rate of liver cancer in the nation.
Why are Asian-Pacific Islanders more prone to getting it than non-Asians? What social, political, economic, and genetic factors help explain why Asians are so at risk? What are considered best practices for addressing hepatitis B – locally, nationally, and internationally? How can community based models like the San Francisco Hep B Free Campaign do a better job of uniting the research, medical, and activist communities in fighting Hep B? These are some of the questions that will be addressed in a landmark public panel discussion on Wednesday September 15, at the Genentech Auditorium on the UCSF Mission Bay Campus located at 600 16th St. in San Francisco.
Featured speakers:
Dr. Baruch Blumberg was the 1976 Nobel Prize in Medicine Recipient for his discovery of the Hepatitis B virus and he later developed a diagnostic test and vaccine against it. He is currently Senior Advisor to the President of Fox Chase Cancer Center, and Professor of Medicine and Anthropology at the University of Pennsylvania. This year, Dr. Blumberg is the 37th recipient of the Chinese Hospital Medical Staff Award.
Ted Fang is the Executive Director of the AsianWeek Foundation and has played a major role in planning, launching and directing the landmark San Francisco Hep B Free Campaign, the largest, most intensive health care campaign for APIs in the U.S.
Fiona Ma (D-San Francisco) is Majority Whip for the California State Assembly and the unofficial chairperson for San Francisco Hep B Free. She, herself is infected with hepatitis B, and is the author of California Assembly Bill 158.
Dr. Marion Peters (moderator) is Professor of Medicine and Chief of Hepatology Research at the U.C. San Francisco, where she holds the John V. Carbone, MD, Endowed Chair in Medicine. Her research focuses on Hepatitis B and C and she is very active in the Hep B Free Campaign.
Dr. Samuel So is the director of the Asian Liver Center at Stanford University, the first non-profit organization in the U.S. that addresses the high incidence of hepatitis B and liver cancer in Asians and Asian Americans. ALC is a founding Steering Committee member of SF Hep B Free and an international expert on hepatitis B.
Co-sponsored by AsianWeek Foundation, Cathay Post #384 Chinese American Veterans, Chinese Hospital, Laotian American National Alliance, San Francisco Hepatitis B Collaborative (UCSF), and Wells Fargo Asian Connection.
To register, please call 415-421-8707; or visit https://secure.acceptiva.com/?cst=ffa8c4
WHEN:
Wednesday, September 15, 2010
5:30 pm Registration
6:00 pm Program
WHERE:
Genentech Auditorium
UCSF Mission Bay Campus
600 16th St.
San Francisco, CA
COST:
Students/Asia Society members $8
Non-members $15
Ten percent of Asian & Pacific Islanders in the United States have chronic hepatitis B. With its sizable API population, nowhere is the HBV epidemic more pronounced and visible than in the Bay Area, which has the highest rate of liver cancer in the nation.Why are Asian-Pacific Islanders more prone to getting it than non-Asians? What social, political, economic, and genetic factors help explain why Asians are so at risk? What are considered best practices for addressing hepatitis B – locally, nationally, and internationally? How can community based models like the San Francisco Hep B Free Campaign do a better job of uniting the research, medical, and activist communities in fighting Hep B? These are some of the questions that will be addressed in a landmark public panel discussion on Wednesday September 15, at the Genentech Auditorium on the UCSF Mission Bay Campus located at 600 16th St. in San Francisco.
Featured speakers:
Dr. Baruch Blumberg was the 1976 Nobel Prize in Medicine Recipient for his discovery of the Hepatitis B virus and he later developed a diagnostic test and vaccine against it. He is currently Senior Advisor to the President of Fox Chase Cancer Center, and Professor of Medicine and Anthropology at the University of Pennsylvania. This year, Dr. Blumberg is the 37th recipient of the Chinese Hospital Medical Staff Award.
Ted Fang is the Executive Director of the AsianWeek Foundation and has played a major role in planning, launching and directing the landmark San Francisco Hep B Free Campaign, the largest, most intensive health care campaign for APIs in the U.S.
Fiona Ma (D-San Francisco) is Majority Whip for the California State Assembly and the unofficial chairperson for San Francisco Hep B Free. She, herself is infected with hepatitis B, and is the author of California Assembly Bill 158.
Dr. Marion Peters (moderator) is Professor of Medicine and Chief of Hepatology Research at the U.C. San Francisco, where she holds the John V. Carbone, MD, Endowed Chair in Medicine. Her research focuses on Hepatitis B and C and she is very active in the Hep B Free Campaign.
Dr. Samuel So is the director of the Asian Liver Center at Stanford University, the first non-profit organization in the U.S. that addresses the high incidence of hepatitis B and liver cancer in Asians and Asian Americans. ALC is a founding Steering Committee member of SF Hep B Free and an international expert on hepatitis B.
Co-sponsored by AsianWeek Foundation, Cathay Post #384 Chinese American Veterans, Chinese Hospital, Laotian American National Alliance, San Francisco Hepatitis B Collaborative (UCSF), and Wells Fargo Asian Connection.
To register, please call 415-421-8707; or visit https://secure.acceptiva.com/?cst=ffa8c4
WHEN:
Wednesday, September 15, 2010
5:30 pm Registration
6:00 pm Program
WHERE:
Genentech Auditorium
UCSF Mission Bay Campus
600 16th St.
San Francisco, CA
COST:
Students/Asia Society members $8
Non-members $15
Monday, August 30, 2010
FOR IMMEDIATE RELEASE: Nobel Laureate Dr. Baruch Blumberg To Be Honored By San Francisco's Hepatitis B Community
Discoverer of Hepatitis B Virus & Developer of Hepatitis B Vaccine
SAN FRANCISCO (August 30, 2010) –Nobel Laureate Dr. Baruch Blumberg who discovered the Hepatitis B Virus and developed the Hepatitis Vaccine will be honored by the Chinese Hospital and San Francisco’s Hepatitis B community. The honor will take place at the Hep B Free Coast to Coast dinner on September 16 at the Regency Grand Ballroom. For ticket or sponsorship information, please go to http://sfhepbfree.org/gala/.
San Francisco’s Hep B Free has created an innovative ecosystem which includes over 50 private and public organizations whose goal is to turn San Francisco into the first hepatitis B city nationwide. Their successful public health model has inspired a national Hep B Free movement from coast to coast.
The 37th Annual Award will be bestowed by the Chinese Hospital in recognition of Dr. Blumberg’s contribution to improving the health of Asians. The night's event is presented by SF Hep B Free and Chinese Hospital, and produced by the AsianWeek Foundation. Past notable awardees include Dr. Samuel So, Director, Asian Liver Center at Stanford University, Dr. David Ho, Director of the Aaron Diamond AIDS Research Center and Dr. James Y. Suen, Professor and Chairman of the Department of Otolaryngology, University of Arkansas & President Bill Clinton’s personal physician.
“As one of the first institutions in the U.S, to provide community screenings for Hepatitis B, honoring Dr. Blumberg is particularly meaningful for us,” said Dr. Joseph Woo, Chief of Staff, Chinese Hospital. “Without Dr. Blumberg’s extraordinary discovery, we would not have been able to help our community and save lives.”
Blumberg received the 1976 Nobel Prize in medicine for his discovery of the Hepatitis B Virus, and in the development of the first vaccine to fight Hepatitis B. His research has had a major impact on worldwide public health. Blumberg is a professor of medicine and anthropology at the University of Pennsylvania and Distinguished Scientist at the Fox Chase Cancer Center in Philadelphia. More recently, he has been involved in research at the National Aeronautics and Space Administration, where he is director of the NASA Astrobiology Institute, which studies the origin, evolution, distribution and future of life in the universe.
“The means are available to prevent and treat Hepatitis B Virus infection,” said Blumberg. “These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are educated about the virus and take part in the program of vaccination, detection, and treatment. The Chinese Hospital, Hep B Free Campaign in San Francisco, along with others such as those of the Hepatitis B Foundation in Pennsylvania and other Hep B free initiatives across the nation are making the public aware of the problem and leading the efforts to solve it.”
Recently, the World Health Organization passed a resolution to mark World Hepatitis Day on July 28, Blumberg’s birthday.
About Hepatitis B (source: Centers for Disease Control and Prevention)
There are more than 43,000 new Hepatitis B cases in United States each year, with the greatest incidence among adults between ages 19–49 years old.Hepatitis B is one of the leading health disparities between Asians and non-Hispanic whites.Among the Asian population the predominant mode of transmission is from infected mother to child during the birthing process. Hepatitis B can also be spread through unprotected sex and shared needles.There is a safe and effective vaccine to protect against infection from Hepatitis B.
About Chinese Hospital
Chinese Hospital, a community-owned, not-for-profit organization, exists primarily to deliver quality health care in a cost effective way, responsive to the community's ethnic and cultural uniqueness. The hospital provides access to health care and acceptability to all socioeconomic levels. Chinese Hospital is governed by a voluntary Board of Trustees, broadly representative of the community, and strives to assume a leadership role in all health matters. For more info, go to http://www.chinesehospital-sf.org.
About AsianWeek Foundation
AsianWeek Foundationis a 501(c)(3) nonprofit organization whose mission is to promote and develop Asian Pacific American identity, community and diversity. AWF does this by bringing people together through cultural events, media campaigns, consulting and innovative programs. AWF encourages the sharing of differences and appreciation of diversity, and works to strengthen relations between all Asian and Pacific Islander cultures, newer and older generations of Asian Pacific Americans, and Asians and non-Asians.
About San Francisco Hep B Free
San Francisco Hep B Free is a first-of-its-kind collaboration between city government, private healthcare community organizations and businesses. The campaign’s goal is to make San Francisco Hepatitis B-free by (1) creating public and healthcare provider awareness about the importance of testing & vaccinating Asian and Pacific Islanders for Hepatitis B; (2) promoting routine Hepatitis B screenings and vaccinations within the primary care medical community; and (3) facilitating access to treatment for chronically infected individuals. The SF Hep B Free Steering Committee is made up of the San Francisco Department of Public Health, the Asian Liver Center at Stanford University and the Asian Week Foundation. For more info, please go to www.sfhepbfree.org.
###
Media Contact:
Grace Niwa, Niwa Public Relations
(617) 299-9848
grace@niwapr.com
SAN FRANCISCO (August 30, 2010) –Nobel Laureate Dr. Baruch Blumberg who discovered the Hepatitis B Virus and developed the Hepatitis Vaccine will be honored by the Chinese Hospital and San Francisco’s Hepatitis B community. The honor will take place at the Hep B Free Coast to Coast dinner on September 16 at the Regency Grand Ballroom. For ticket or sponsorship information, please go to http://sfhepbfree.org/gala/.
San Francisco’s Hep B Free has created an innovative ecosystem which includes over 50 private and public organizations whose goal is to turn San Francisco into the first hepatitis B city nationwide. Their successful public health model has inspired a national Hep B Free movement from coast to coast.
The 37th Annual Award will be bestowed by the Chinese Hospital in recognition of Dr. Blumberg’s contribution to improving the health of Asians. The night's event is presented by SF Hep B Free and Chinese Hospital, and produced by the AsianWeek Foundation. Past notable awardees include Dr. Samuel So, Director, Asian Liver Center at Stanford University, Dr. David Ho, Director of the Aaron Diamond AIDS Research Center and Dr. James Y. Suen, Professor and Chairman of the Department of Otolaryngology, University of Arkansas & President Bill Clinton’s personal physician.
“As one of the first institutions in the U.S, to provide community screenings for Hepatitis B, honoring Dr. Blumberg is particularly meaningful for us,” said Dr. Joseph Woo, Chief of Staff, Chinese Hospital. “Without Dr. Blumberg’s extraordinary discovery, we would not have been able to help our community and save lives.”
Blumberg received the 1976 Nobel Prize in medicine for his discovery of the Hepatitis B Virus, and in the development of the first vaccine to fight Hepatitis B. His research has had a major impact on worldwide public health. Blumberg is a professor of medicine and anthropology at the University of Pennsylvania and Distinguished Scientist at the Fox Chase Cancer Center in Philadelphia. More recently, he has been involved in research at the National Aeronautics and Space Administration, where he is director of the NASA Astrobiology Institute, which studies the origin, evolution, distribution and future of life in the universe.
“The means are available to prevent and treat Hepatitis B Virus infection,” said Blumberg. “These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are educated about the virus and take part in the program of vaccination, detection, and treatment. The Chinese Hospital, Hep B Free Campaign in San Francisco, along with others such as those of the Hepatitis B Foundation in Pennsylvania and other Hep B free initiatives across the nation are making the public aware of the problem and leading the efforts to solve it.”
Recently, the World Health Organization passed a resolution to mark World Hepatitis Day on July 28, Blumberg’s birthday.
About Hepatitis B (source: Centers for Disease Control and Prevention)
There are more than 43,000 new Hepatitis B cases in United States each year, with the greatest incidence among adults between ages 19–49 years old.Hepatitis B is one of the leading health disparities between Asians and non-Hispanic whites.Among the Asian population the predominant mode of transmission is from infected mother to child during the birthing process. Hepatitis B can also be spread through unprotected sex and shared needles.There is a safe and effective vaccine to protect against infection from Hepatitis B.
About Chinese Hospital
Chinese Hospital, a community-owned, not-for-profit organization, exists primarily to deliver quality health care in a cost effective way, responsive to the community's ethnic and cultural uniqueness. The hospital provides access to health care and acceptability to all socioeconomic levels. Chinese Hospital is governed by a voluntary Board of Trustees, broadly representative of the community, and strives to assume a leadership role in all health matters. For more info, go to http://www.chinesehospital-sf.org.
About AsianWeek Foundation
AsianWeek Foundationis a 501(c)(3) nonprofit organization whose mission is to promote and develop Asian Pacific American identity, community and diversity. AWF does this by bringing people together through cultural events, media campaigns, consulting and innovative programs. AWF encourages the sharing of differences and appreciation of diversity, and works to strengthen relations between all Asian and Pacific Islander cultures, newer and older generations of Asian Pacific Americans, and Asians and non-Asians.
About San Francisco Hep B Free
San Francisco Hep B Free is a first-of-its-kind collaboration between city government, private healthcare community organizations and businesses. The campaign’s goal is to make San Francisco Hepatitis B-free by (1) creating public and healthcare provider awareness about the importance of testing & vaccinating Asian and Pacific Islanders for Hepatitis B; (2) promoting routine Hepatitis B screenings and vaccinations within the primary care medical community; and (3) facilitating access to treatment for chronically infected individuals. The SF Hep B Free Steering Committee is made up of the San Francisco Department of Public Health, the Asian Liver Center at Stanford University and the Asian Week Foundation. For more info, please go to www.sfhepbfree.org.
###
Media Contact:
Grace Niwa, Niwa Public Relations
(617) 299-9848
grace@niwapr.com
Friday, August 27, 2010
Nobel Laureate Dr. Baruch Blumberg To Be Honored By San Francisco�s Hepatitis B Community
Article on U.S. ASIAN WIRE
Discoverer of Hepatitis B Virus & Developer of Hepatitis B Vaccine
August 27, 2010
SAN FRANCISCO -- (U.S. ASIAN WIRE) -- Nobel Laureate Dr. Baruch Blumberg who discovered the Hepatitis B Virus and developed the Hepatitis Vaccine will be honored by the Chinese Hospital and San Francisco's hepatitis B community. The honor will take place at the Hep B Free Coast to Coast dinner on September 16 at the Regency Grand Ballroom. For ticket or sponsorship information, please go to http://www.sfhepbfree.org/gala/.
San Francisco's Hep B Free has created an innovative ecosystem which includes over 50 private and public organizations whose goal is to turn San Francisco into the first hepatitis B city nationwide. Their successful public health model has inspired a national Hep B Free movement from coast to coast.
The 37th Annual Award will be bestowed by the Chinese Hospital in recognition of Dr. Blumberg's contribution to improving the health of Asians. The night's event is presented by SF Hep B Free and Chinese Hospital, and produced by the AsianWeek Foundation. Past notable awardees include Dr. Samuel So, Director, Asian Liver Center at Stanford University, Dr. David Ho, Director of the Aaron Diamond AIDS Research Center and Dr. James Y. Suen, Professor and Chairman of the Department of Otolaryngology, University of Arkansas & President Bill Clinton's personal physician.
"As one of the first institutions in the U.S, to provide community screenings for Hepatitis B, honoring Dr. Blumberg is particularly meaningful for us," said Dr. Joseph Woo, Chief of Staff, Chinese Hospital. "Without Dr. Blumberg's extraordinary discovery, we would not have been able to help our community and save lives."
Blumberg received the 1976 Nobel Prize in medicine for his discovery of the Hepatitis B Virus, and in the development of the first vaccine to fight Hepatitis B. His research has had a major impact on worldwide public health. Blumberg is a professor of medicine and anthropology at the University of Pennsylvania and Distinguished Scientist at the Fox Chase Cancer Center in Philadelphia. More recently, he has been involved in research at the National Aeronautics and Space Administration, where he is director of the NASA Astrobiology Institute, which studies the origin, evolution, distribution and future of life in the universe.
"The means are available to prevent and treat Hepatitis B Virus infection," said Blumberg. "These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are educated about the virus and take part in the program of vaccination, detection, and treatment. The Chinese Hospital, Hep B Free Campaign in San Francisco, along with others such as those of the Hepatitis B Foundation in Pennsylvania and other Hep B free initiatives across the nation are making the public aware of the problem and leading the efforts to solve it."
Recently, the World Health Organization passed a resolution to mark World Hepatitis Day on July 28, Blumberg's birthday.
About Hepatitis B (source: Centers for Disease Control and Prevention)
* There are more than 43,000 new Hepatitis B cases in United States each year, with the greatest incidence among adults between ages 19�49 years old.
* Hepatitis B is one of the leading health disparities between Asians and non-Hispanic whites.
* Among the Asian population the predominant mode of transmission is from infected mother to child during the birthing process. Hepatitis B can also be spread through unprotected sex and shared needles.
* There is a safe and effective vaccine to protect against infection from Hepatitis B.
About Chinese Hospital
Chinese Hospital, a community-owned, not-for-profit organization, exists primarily to deliver quality health care in a cost effective way, responsive to the community's ethnic and cultural uniqueness. The hospital provides access to health care and acceptability to all socioeconomic levels. Chinese Hospital is governed by a voluntary Board of Trustees, broadly representative of the community, and strives to assume a leadership role in all health matters. For more info, go to http://www.chinesehospital-sf.org.
About AsianWeek Foundation
AsianWeek Foundation is a 501(c)(3) nonprofit organization whose mission is to promote and develop Asian Pacific American identity, community and diversity. AWF does this by bringing people together through cultural events, media campaigns, consulting and innovative programs. AWF encourages the sharing of differences and appreciation of diversity, and works to strengthen relations between all Asian and Pacific Islander cultures, newer and older generations of Asian Pacific Americans, and Asians and non-Asians.
About San Francisco Hep B Free
San Francisco Hep B Free is a first-of-its-kind collaboration between city government, private healthcare community organizations and businesses. The campaign's goal is to make San Francisco Hepatitis B-free by (1) creating public and healthcare provider awareness about the importance of testing & vaccinating Asian and Pacific Islanders for Hepatitis B; (2) promoting routine Hepatitis B screenings and vaccinations within the primary care medical community; and (3) facilitating access to treatment for chronically infected individuals. The SF Hep B Free Steering Committee is made up of the San Francisco Department of Public Health, the Asian Liver Center at Stanford University and the Asian Week Foundation. For more info, please go to www.sfhepbfree.org.
Contact:
Grace Niwa, Niwa Public Relations
646-644-5799
grace@niwapr.com
Discoverer of Hepatitis B Virus & Developer of Hepatitis B Vaccine
August 27, 2010
SAN FRANCISCO -- (U.S. ASIAN WIRE) -- Nobel Laureate Dr. Baruch Blumberg who discovered the Hepatitis B Virus and developed the Hepatitis Vaccine will be honored by the Chinese Hospital and San Francisco's hepatitis B community. The honor will take place at the Hep B Free Coast to Coast dinner on September 16 at the Regency Grand Ballroom. For ticket or sponsorship information, please go to http://www.sfhepbfree.org/gala/.
San Francisco's Hep B Free has created an innovative ecosystem which includes over 50 private and public organizations whose goal is to turn San Francisco into the first hepatitis B city nationwide. Their successful public health model has inspired a national Hep B Free movement from coast to coast.
The 37th Annual Award will be bestowed by the Chinese Hospital in recognition of Dr. Blumberg's contribution to improving the health of Asians. The night's event is presented by SF Hep B Free and Chinese Hospital, and produced by the AsianWeek Foundation. Past notable awardees include Dr. Samuel So, Director, Asian Liver Center at Stanford University, Dr. David Ho, Director of the Aaron Diamond AIDS Research Center and Dr. James Y. Suen, Professor and Chairman of the Department of Otolaryngology, University of Arkansas & President Bill Clinton's personal physician.
"As one of the first institutions in the U.S, to provide community screenings for Hepatitis B, honoring Dr. Blumberg is particularly meaningful for us," said Dr. Joseph Woo, Chief of Staff, Chinese Hospital. "Without Dr. Blumberg's extraordinary discovery, we would not have been able to help our community and save lives."
Blumberg received the 1976 Nobel Prize in medicine for his discovery of the Hepatitis B Virus, and in the development of the first vaccine to fight Hepatitis B. His research has had a major impact on worldwide public health. Blumberg is a professor of medicine and anthropology at the University of Pennsylvania and Distinguished Scientist at the Fox Chase Cancer Center in Philadelphia. More recently, he has been involved in research at the National Aeronautics and Space Administration, where he is director of the NASA Astrobiology Institute, which studies the origin, evolution, distribution and future of life in the universe.
"The means are available to prevent and treat Hepatitis B Virus infection," said Blumberg. "These good outcomes can only be fully achieved if the public, and particularly populations with a high rate of infection, including those of Asian origin, are educated about the virus and take part in the program of vaccination, detection, and treatment. The Chinese Hospital, Hep B Free Campaign in San Francisco, along with others such as those of the Hepatitis B Foundation in Pennsylvania and other Hep B free initiatives across the nation are making the public aware of the problem and leading the efforts to solve it."
Recently, the World Health Organization passed a resolution to mark World Hepatitis Day on July 28, Blumberg's birthday.
About Hepatitis B (source: Centers for Disease Control and Prevention)
* There are more than 43,000 new Hepatitis B cases in United States each year, with the greatest incidence among adults between ages 19�49 years old.
* Hepatitis B is one of the leading health disparities between Asians and non-Hispanic whites.
* Among the Asian population the predominant mode of transmission is from infected mother to child during the birthing process. Hepatitis B can also be spread through unprotected sex and shared needles.
* There is a safe and effective vaccine to protect against infection from Hepatitis B.
About Chinese Hospital
Chinese Hospital, a community-owned, not-for-profit organization, exists primarily to deliver quality health care in a cost effective way, responsive to the community's ethnic and cultural uniqueness. The hospital provides access to health care and acceptability to all socioeconomic levels. Chinese Hospital is governed by a voluntary Board of Trustees, broadly representative of the community, and strives to assume a leadership role in all health matters. For more info, go to http://www.chinesehospital-sf.org.
About AsianWeek Foundation
AsianWeek Foundation is a 501(c)(3) nonprofit organization whose mission is to promote and develop Asian Pacific American identity, community and diversity. AWF does this by bringing people together through cultural events, media campaigns, consulting and innovative programs. AWF encourages the sharing of differences and appreciation of diversity, and works to strengthen relations between all Asian and Pacific Islander cultures, newer and older generations of Asian Pacific Americans, and Asians and non-Asians.
About San Francisco Hep B Free
San Francisco Hep B Free is a first-of-its-kind collaboration between city government, private healthcare community organizations and businesses. The campaign's goal is to make San Francisco Hepatitis B-free by (1) creating public and healthcare provider awareness about the importance of testing & vaccinating Asian and Pacific Islanders for Hepatitis B; (2) promoting routine Hepatitis B screenings and vaccinations within the primary care medical community; and (3) facilitating access to treatment for chronically infected individuals. The SF Hep B Free Steering Committee is made up of the San Francisco Department of Public Health, the Asian Liver Center at Stanford University and the Asian Week Foundation. For more info, please go to www.sfhepbfree.org.
Contact:
Grace Niwa, Niwa Public Relations
646-644-5799
grace@niwapr.com
Monday, July 26, 2010
Health, Community Leaders in San Francisco Campaign Against Hepatitis B
Rachel Silverman | San Francisco, VOANews.com
 Public health officials in San Francisco, and leaders from its large Asian community, are mounting an aggressive campaign to eradicate hepatitis B from the city. They say demographics are largely responsible for San Francisco having the highest concentration of hepatitis B in the U.S, as well as the highest rates of liver cancer, which is usually caused by the virus.
Public health officials in San Francisco, and leaders from its large Asian community, are mounting an aggressive campaign to eradicate hepatitis B from the city. They say demographics are largely responsible for San Francisco having the highest concentration of hepatitis B in the U.S, as well as the highest rates of liver cancer, which is usually caused by the virus.
Greg Zhang, 46, is recovering from recent surgery to remove a tumor from his liver...a result of his life-long infection with hepatitis B.
Zhang's surgeon is Dr. Samuel So, director of the Stanford University Asian Liver Center.
"Hepatitis B is the silent killer because most people who are chronically infected may not be aware of the infection," he said. "In fact you know two out of three of them don't even know they're infected because usually they feel perfectly healthy."
The hepatitis B virus is found in blood and bodily fluids. Many people can live with the virus and never get sick, but 25 percent of those infected eventually develop severe liver damage or cancer. The virus can be transmitted by unsafe sex and unsterile needles, but most people who suffer from the disease become infected at birth from their mothers.
Zhang, and his younger brother Haiyang, were born in China, one of several Asian countries where the disease is endemic. Haiyang died of advanced liver cancer shortly after he was diagnosed.
The American Liver Foundation says one in 10 Asian Americans have the virus, a disease that's 100 times more likely to strike Asian Americans than other ethnic groups. And in San Francisco, a full one-third of the population is of Asian descent.
The city's Hep B Free Campaign offers free testing, vaccinations, and treatment. There's no known cure for hepatitis B, although the virus can be kept in check with anti-viral medicines. Those infected need to have yearly ultrasounds and blood tests to screen for early stages of liver cancer.
Newborns need a vaccination within the first day of life to prevent transmission of the virus from their mothers, and babies need two more doses within the first six months for full immunity.
Public awareness is another part of the campaign. A controversial advertisement on television and billboards shows 10 Asian beauty pageant contestants and asks which one deserves to die.
Hepatitis B carries a stigma. And that is something California Assembly member Fiona Ma of San Francisco is working hard to change. She is Hepatitis B-positive.
"My cousin, who was born in China, actually got very upset and said, 'Please don't talk about it. People will think you are sick and they are not going to vote for you.' And my message was, 'I am a public figure and this is my responsibility,'" she said.
But Stanford's Dr. So - whose mother-in-law died from liver cancer - says changing attitudes is just a start. He says other diseases get more public attention and therefore more money.
"This is really tragic on a global scale, there's really major neglect about hepatitis B. About one in 20 people in the world are chronically infected. One in 20. Ten times more than people in the world infected with HIV," Dr. So said.
For now, the battle against hepatitis B is concentrated in communities with large Asian populations. Other cities, including Philadelphia, Washington and Los Angeles, are making plans to use the San Francisco program as a model.
Public health officials in San Francisco, and leaders from its large Asian community, are mounting an aggressive campaign to eradicate hepatitis B from the city. They say demographics are largely responsible for San Francisco having the highest concentration of hepatitis B in the U.S, as well as the highest rates of liver cancer, which is usually caused by the virus.Greg Zhang, 46, is recovering from recent surgery to remove a tumor from his liver...a result of his life-long infection with hepatitis B.
Zhang's surgeon is Dr. Samuel So, director of the Stanford University Asian Liver Center.
"Hepatitis B is the silent killer because most people who are chronically infected may not be aware of the infection," he said. "In fact you know two out of three of them don't even know they're infected because usually they feel perfectly healthy."
The hepatitis B virus is found in blood and bodily fluids. Many people can live with the virus and never get sick, but 25 percent of those infected eventually develop severe liver damage or cancer. The virus can be transmitted by unsafe sex and unsterile needles, but most people who suffer from the disease become infected at birth from their mothers.
Zhang, and his younger brother Haiyang, were born in China, one of several Asian countries where the disease is endemic. Haiyang died of advanced liver cancer shortly after he was diagnosed.
The American Liver Foundation says one in 10 Asian Americans have the virus, a disease that's 100 times more likely to strike Asian Americans than other ethnic groups. And in San Francisco, a full one-third of the population is of Asian descent.
The city's Hep B Free Campaign offers free testing, vaccinations, and treatment. There's no known cure for hepatitis B, although the virus can be kept in check with anti-viral medicines. Those infected need to have yearly ultrasounds and blood tests to screen for early stages of liver cancer.
Newborns need a vaccination within the first day of life to prevent transmission of the virus from their mothers, and babies need two more doses within the first six months for full immunity.
Public awareness is another part of the campaign. A controversial advertisement on television and billboards shows 10 Asian beauty pageant contestants and asks which one deserves to die.
Hepatitis B carries a stigma. And that is something California Assembly member Fiona Ma of San Francisco is working hard to change. She is Hepatitis B-positive.
"My cousin, who was born in China, actually got very upset and said, 'Please don't talk about it. People will think you are sick and they are not going to vote for you.' And my message was, 'I am a public figure and this is my responsibility,'" she said.
But Stanford's Dr. So - whose mother-in-law died from liver cancer - says changing attitudes is just a start. He says other diseases get more public attention and therefore more money.
"This is really tragic on a global scale, there's really major neglect about hepatitis B. About one in 20 people in the world are chronically infected. One in 20. Ten times more than people in the world infected with HIV," Dr. So said.
For now, the battle against hepatitis B is concentrated in communities with large Asian populations. Other cities, including Philadelphia, Washington and Los Angeles, are making plans to use the San Francisco program as a model.
Friday, July 2, 2010
Hepatitis B: An Asian-American Plague?
by Chris Santiago | Change.org
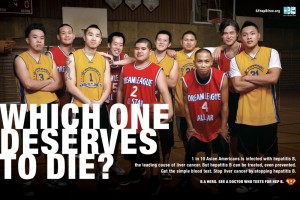 "In the Asian-American family, usually parents don't want to discuss if they have diseases," Albert Ng recently told NPR while attending San Francisco's Asian Heritage Street Fair. "They just want to discuss the good stuff, but never discuss the weaknesses."
"In the Asian-American family, usually parents don't want to discuss if they have diseases," Albert Ng recently told NPR while attending San Francisco's Asian Heritage Street Fair. "They just want to discuss the good stuff, but never discuss the weaknesses."
Ng was at a booth getting tested for hepatitis B for the first time in his life. One in 10 Asian-Americans is chronically infected with the disease; when left untreated, hepatitis B can lead to liver cancer. San Francisco has the highest liver cancer rate in the country, and this is mostly due to the city's famously large population of Asian-Americans, for whom hep B has become an epidemic. Of the 1.25 million Americans who are affected by hep B, half are Asian-Americans.
Why is hepatitis B so common among Asians? The disease is thought to have originated in Asia centuries ago. It's passed down from infected mothers to newborn infants. While blood tests can detect the hep B virus, most physicians in the U.S. only test those who engage in high-risk behaviors, such as unprotected sex or intravenous drug use. Many doctors simply aren't aware that Asian immigrants, especially those from China, are much more likely to have been infected at birth.
To make matters worse, many Asian-Americans who could have been infected at birth may be completely in the dark about the matter. As Ng pointed out to NPR, traditional Asian values may be partly to blame: It's not unlikely that Asian immigrants who knew they were infected with hep B regarded that fact as something shameful, as something that was better not to be discussed.
Some Asian-Americans that I know well also take a fatalistic attitude toward histories of hep B and liver cancer in their families. "If it's going to happen, it's going to happen," is how the conversation often turns. "Better to live your life without worrying about it."
The thing is, hep B can be suppressed with medication, if it's caught early.
"This is a disease [for] which, unlike HIV, we have all the solutions," Samuel So, director of the Asian Liver Center at Stanford University, told NPR. "We know how to prevent it. We have a very effective vaccine; we have treatments which can help to suppress the virus, and yet we are not doing a good job."
Which brings us back to Albert Ng: In addition to a hard-hitting public awareness campaign, city health officials in San Francisco have begun offering free testing, vaccination and treatment to all residents. Ng was getting tested because it turns out that his own grandfather died of liver cancer caused by hepatitis B.
Nationwide, liver cancer and hep B are becoming an Asian-American epidemic. To combat this epidemic, the community needs to talk, and it also needs to shake a few trees. Take the city of New York, for example: 12% of the population of New York is Asian-American. But as recently as 2008, less than one percent of social services were channeled toward the Asian-American community. According to the Coaltion for Asian American Children & Families, Asian-Americans were 10 times as likely to develop liver cancer as the rest of the population of New York.
San Francisco's program is promising, and other cities plan to replicate its efforts. But to combat liver cancer and hep B, we're going to need to raise money — and our voices.
Photo Credit: San Francisco Hep B Free
Chris Santiago is a freelance writer and editor who until recently was an editor at McGraw-Hill.
Ng was at a booth getting tested for hepatitis B for the first time in his life. One in 10 Asian-Americans is chronically infected with the disease; when left untreated, hepatitis B can lead to liver cancer. San Francisco has the highest liver cancer rate in the country, and this is mostly due to the city's famously large population of Asian-Americans, for whom hep B has become an epidemic. Of the 1.25 million Americans who are affected by hep B, half are Asian-Americans.
Why is hepatitis B so common among Asians? The disease is thought to have originated in Asia centuries ago. It's passed down from infected mothers to newborn infants. While blood tests can detect the hep B virus, most physicians in the U.S. only test those who engage in high-risk behaviors, such as unprotected sex or intravenous drug use. Many doctors simply aren't aware that Asian immigrants, especially those from China, are much more likely to have been infected at birth.
To make matters worse, many Asian-Americans who could have been infected at birth may be completely in the dark about the matter. As Ng pointed out to NPR, traditional Asian values may be partly to blame: It's not unlikely that Asian immigrants who knew they were infected with hep B regarded that fact as something shameful, as something that was better not to be discussed.
Some Asian-Americans that I know well also take a fatalistic attitude toward histories of hep B and liver cancer in their families. "If it's going to happen, it's going to happen," is how the conversation often turns. "Better to live your life without worrying about it."
The thing is, hep B can be suppressed with medication, if it's caught early.
"This is a disease [for] which, unlike HIV, we have all the solutions," Samuel So, director of the Asian Liver Center at Stanford University, told NPR. "We know how to prevent it. We have a very effective vaccine; we have treatments which can help to suppress the virus, and yet we are not doing a good job."
Which brings us back to Albert Ng: In addition to a hard-hitting public awareness campaign, city health officials in San Francisco have begun offering free testing, vaccination and treatment to all residents. Ng was getting tested because it turns out that his own grandfather died of liver cancer caused by hepatitis B.
Nationwide, liver cancer and hep B are becoming an Asian-American epidemic. To combat this epidemic, the community needs to talk, and it also needs to shake a few trees. Take the city of New York, for example: 12% of the population of New York is Asian-American. But as recently as 2008, less than one percent of social services were channeled toward the Asian-American community. According to the Coaltion for Asian American Children & Families, Asian-Americans were 10 times as likely to develop liver cancer as the rest of the population of New York.
San Francisco's program is promising, and other cities plan to replicate its efforts. But to combat liver cancer and hep B, we're going to need to raise money — and our voices.
Photo Credit: San Francisco Hep B Free
Chris Santiago is a freelance writer and editor who until recently was an editor at McGraw-Hill.
Wednesday, June 30, 2010
ABC7: "Beyond the Headlines: Asian Roundtable"
ABC7's Emmy award-winning public affairs show, "Beyond the Headlines," provides in-depth coverage of the topics and issues facing the people of the Bay Area. Throughout the year, "Beyond the Headlines" airs half-hour specials on issues, ranging from Bay Area housing to same-sex marriage.
http://abclocal.go.com/kgo/video?id=7526520
BEYOND THE HEADLINES
June 27, 2010
Hosted by ABC7's Kristen Sze
This week's show looks at our Asian American community. We invited four Bay Area leaders representing various fields, to talk about being Asian American today, and the opportunities and challenges facing the community.
Let's begin with a snapshot of the population. According to the U.S. Census Bureau, the Census in 2000 found that:
- There are close to 12 million Asians living in the United States.
- That's 4.2% of the entire population.
- California has the largest Asian population, with 4.2 million.
- Of the nation's largest cities with a population of 100,000 or greater, the Bay Area has the highest percentage of Asians.
Topics covered include:
* Leadership
* Business
* Politics
* Media and the Arts, Stereotypes
* Hepatitis B and Health Disparities
* Current Issues
Studio Guests:
Charles Huang
Co-Founder and Executive Vice-President, Guitar Hero
www.guitarherocorp.com/about.php
Kyung Yoon
Founder/CEO, Talent Age Associates
www.talentage.com/about_bios.html
Fiona Ma
Assembly Member, District 12
democrats.assembly.ca.gov/members/a12/
415-557-2312
Jeff Adachi
San Francisco Public Defender
sfpublicdefender.org
415-553-1671
Sunday, June 27, 2010
San Francisco HepBfree Campaign serves as model for Philadelphia HepBfree
San Francisco HepBfree Campaign serves as model for Philadelphia HepBfree:
Thursday, June 17, 2010
Howard Koh Testimony before Committee on Oversight and Governmental Reform, U.S. House of Representatives
View full article on HHS.gov website
Statement by Howard K Koh, M.D., M.P.H.,
Assistant Secretary for Health
U.S. Department of Health and Human Services (HHS)
on
Viral Hepatitis: The Secret Epidemic
before
Committee on Oversight and Governmental Reform
United States House of Representatives
Thursday, June 17, 2010
Good morning, Chairman Towns, Ranking Member Issa, and other distinguished Members of the Committee. I am Dr. Howard Koh, the Assistant Secretary for Health in the Department of Health and Human Services (HHS or the Department). I am honored to be here today to discuss the silent epidemic of viral hepatitis in this country, and the coordinated steps the Department is taking to effectively address this significant public health problem through better prevention, care and monitoring efforts.
Viral hepatitis is a collective term describing liver inflammation or hepatitis caused by a group of several different viruses. Three viruses, Hepatitis A virus (HAV), Hepatitis B virus (HBV) and Hepatitis C virus (HCV) cause most viral hepatitis in the United States. Spread in unsanitary conditions, hepatitis A cases have declined significantly in the U.S. in recent years as a result of vaccination programs and food safety efforts. Today, I will focus my remarks on the prevention of HBV and HCV transmission and associated morbidity and mortality. Unlike HAV, HBV and HCV infections are blood-borne and often persist for years, resulting in ongoing (chronic) but usually asymptomatic liver inflammation, and in some cases scarring (cirrhosis) that leads to liver failure and/or and liver cancer. Chronic hepatitis is a major cause of liver cancer and chronic liver disease globally and in the United States.
HBV and HCV Disease Burden
Worldwide, 480 million to 540 million persons are living with chronic viral hepatitis, with 350 million 1, 2 to 370 3 million infected with HBV and 130 million to 170 million infected with HCV.4
All told, chronic viral hepatitis afflicts about 1 in every 12 persons worldwide. About 54,000 persons with chronic hepatitis B infections immigrate to the U.S. annually. Chronic hepatitis causes considerable morbidity. Globally, an estimated 78% of primary liver cancer and 57% of liver cirrhosis are caused by chronic viral hepatitis and about one million deaths from viral hepatitis occur each year.4 Liver cancer is the fourth -leading cause of death from cancer worldwide, the third -leading cause among men.5 The most recent liver cancer surveillance data indicate that long-term liver cancer incidence is increasing in the U.S., with an average annual percentage change in incidence between 2001 and 2006 of 3.5% per year.6
In the United States, viral hepatitis remains no less of a problem; 3.5 million to 5.3 million Americans have chronic viral hepatitis. 7, 8, 9 The vast majority, an estimated 65 % and 75% are not aware they are infected with HBV and HCV, respectively. 7 In the absence of appropriate treatment, 15-40% of infected persons will develop liver cirrhosis. 10, 11, 12 Viral hepatitis is the leading cause of liver transplantation in the United States. 13 Co-factors, including HIV, excessive alcohol use, and fatty liver disease associated with obesity and diabetes, amplify the effects of viral hepatitis, hastening development of liver disease. Fifteen to thirty percent of all persons infected with HIV have chronic viral hepatitis, 14 and liver disease is now the main non-AIDS cause of death in HIV-infected persons. 15 In contrast to almost all other types of cancer, liver cancer rates have tripled over the last several decades, 16 fueled in large part by the progression of viral hepatitis to end-stage disease among persons infected years ago. In the United States, viral hepatitis causes 12,000 to 15,000 deaths annually, 17, 18 and viral hepatitis-related illness, deaths, and costs are all expected to rise substantially in the coming years.
Viral hepatitis poses a major health threat for certain populations. Among persons aged 46 to 64 years (i.e., baby boomers), about 1 in 33 have chronic viral hepatitis. 9 One out of every 7 African American men in their 40s is living with chronic hepatitis C, 9 and approximately 1 in 12 Asian Americans is living with chronic hepatitis B. 19 Similarly, the profiles of persons with liver cancer mirror the demographic characteristics of persons with chronic viral hepatitis; liver cancer incidence is highest among Asians/Pacific Islanders, and is increasing among Hispanics, African Americans, baby boomers, and males. 20
New HBV and HCV infections add to the burden of chronic viral hepatitis and liver disease. In 2007, there were an estimated 43,000 new cases of HBV infection. 10 HBV is spread from mother to child at the time of birth, among household contacts through incidental blood exposures in the home, through injection drug use, and through sexual contact. Viral hepatitis transmission should never occur as a result of health care delivery, but transmission has been documented in a variety of health care settings when providers have failed to follow basic infection control practices. Rates of HBV infection are highest among adults, reflecting low hepatitis B vaccination coverage among persons with risks such as injection drug use and multiple sexual partners. Prevention of mother-to-child transmission is critical, as 90% of HBV -infected newborns remain infected 21, 22, 23 and about 1 in 4 die from complications of chronic viral hepatitis in later life. 11 Outbreaks of hepatitis B occur in persons not currently recommended to receive the vaccine, such as persons with diabetes, patients in outpatient settings, and residents of long term care facilities; they also occur in health care settings when providers fail to follow basic infection control.
Surveillance data suggest nearly 20,000 10 persons are newly infected with HCV annually in the United States. HCV is primarily a blood-borne virus spread through injection drug use. Transmission also occurs in health care settings as a result of unacceptable lapses in infection control, primarily related to the misuse of syringes and medication vials. Non-injecting drug users who snort cocaine and other drugs also have elevated risks for HCV, possibly from blood exposure associated with intranasal use. Perhaps typically thought of as an urban disease, HCV transmission has been detected among young drug users in suburban and rural communities. In addition, after reports from Europe for several years, sexual transmission of HCV has been detected among U.S. cohorts of HIV-infected men who have sex with men (MSM). In certain circumstances, HCV can be transmitted sexually and at the time of birth.
Public Health Prevention Measures to Address Viral Hepatitis
Public health measures can prevent transmission. These measures have helped our nation achieve remarkable declines in the number of new infections with both viruses. Safe and effective vaccines are available to provide long term protection from hepatitis B. In 1991, the Centers for Disease Control and Prevention (CDC) and the national Advisory Committee on Immunization Practices (ACIP) set forth an ambitious vaccine-based strategy to eliminate HBV transmission in the United States. 24 This strategy involves vaccinating newborns and older children, as well as vaccinating at-risk adults.
Routine vaccination of infants and catch-up vaccination of older children under federally -supported vaccination programs has successfully driven down rates of HBV transmission and acute cases of disease, with rates falling 82% from 8.5 cases per 100,000 population in 1990 to 1.5 cases per 100,000 population in 2007, the most recent year for which data are available. 10 Rates have declined most dramatically—98%—among children aged 15 years and younger. Vaccine coverage among children aged 19 months to 35 months is 93%. 25, 26
In the United States, approximately 24,000 HBV-infected women give birth each year 27 , most of whom are identified by prenatal screening. Their infants are recommended to receive protective hepatitis B vaccination and other prevention services. State and local prevention programs currently do not have the capacity to manage all of the estimated newborns who are exposed. To assure newborns exposed to HBV are protected, CDC recommends that all infants receive a birth dose of hepatitis B vaccine. In 2008, 55% of newborns received a birth dose in the first three days of life. 30 As not all newborns receive protective interventions, each year hundreds of infants are infected with HBV in the United States. 28
Hepatitis B vaccine is also recommended for adults with sexual and blood exposure risks. As the result of improvements in infection control and ongoing hepatitis B vaccination, relatively few cases now occur in certain populations such as dialysis patients and healthcare workers that previously were considered to be at high risk. However, while the number of new cases has declined among adults, 95 % of all new cases are among adults. A high proportion of those cases occur among persons with risk behaviors such as injecting drug users, MSM, and persons with multiple sex partners. Rates are particularly high among males aged 25 to 44 years old. 10
Unlike HBV, there is no vaccine yet developed for HCV. However, since HCV was discovered in the 1980s, the development of prevention interventions has caused a significant decline in new cases. Screening of donated blood and other tissues and organs now protects recipients of these donations. Screening, together with behavioral education, and access to clean syringes and drug treatment have had a role in reducing the number of new cases of HCV related to injection drug use 8 In addition, the adoption of standard precautions in health care settings has reduced transmission risks for all blood -borne viruses, including HBV and HCV.
The onset of liver cancer and other liver disease can be prevented through screening and care for persons chronically infected with HBV or HCV. Current treatments can halt or even reverse the liver damage caused by viral hepatitis. New treatments on the immediate horizon hold even greater promise for a definitive cure. CDC recommends screening to identify persons with viral hepatitis and prevention and care services to reduce transmission and morbidity.
Prevention and care for viral hepatitis makes economic sense. Published studies estimate that medical costs for viral hepatitis run in the billions of dollars per year. 29, 30 Numerous studies reveal the cost-effective benefits of screening and care for populations at risk for viral hepatitis. 31, 32, 33, 34 Hepatitis screening linked to vaccination and care is a cost -effective prevention approach to eliminating health disparities for Asian and Pacific Island Americans. 35 Preliminary data from a CDC model show that by identifying and referring for appropriate care all HCV-infected persons in primary care, approximately 87,000 cases of end stage liver disease and 11,000 liver transplants can be prevented, and 840,000 undiscounted life years would be gained, with an estimated cost per discounted quality adjusted life year, or QALY, of $43,000. Similarly, preliminary estimates reveal that expanded HBV screening and care could avert approximately 140,000 cases of end stage liver disease and gain 3.3 million QALYs.
The Institute of Medicine Report
In January 2010, The Institute of Medicine (IOM) issued a report titled, Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. The report identified multiple barriers that have combined to create a situation in which inadequate public resources are available to support the prevention, care and monitoring needed to fully and effectively address this important public health problem.
The IOM report described deficiencies that have created adverse consequences for the health of our nation:
* Inadequate disease surveillance systems underreport acute and chronic infections, so the full extent of the problem is unknown;
* At-risk people do not know that they are at risk or how to prevent becoming infected;
* At-risk people may not have access to prevention services;
* Chronically infected people do not know they are infected;
* Many healthcare providers do not screen people for risk factors or do not know how to manage infected people; and
* Infected people often have inadequate access to testing, social support, and medical management services.
The IOM called for an intensified, coordinated national effort to improve the prevention of viral hepatitis and better protect the health of Americans.
The HHS Response to the IOM Report
HHS and its agencies are fully committed to accelerating progress towards the prevention of viral hepatitis and associated disease in the U.S., and advancing this strategy. In January, HHS established an interagency work group on viral hepatitis, which I chair, that has diverse representation from HHS operating divisions. A work group subcommittee is currently drafting a comprehensive strategic action plan for HHS to improve the coordination of viral hepatitis prevention, care and monitoring activities within the Department. The action plan is grouped by focus areas: Increasing community awareness and provider education; strengthening surveillance for viral hepatitis; preventing viral hepatitis transmission through vaccination; preventing blood-borne transmission; and improving clinical preventive care and treatment services. The current timeline is to complete this action plan by October 1, fall 2010.
There are millions of persons who are unaware they have a potentially life -threatening disease. Major goals of viral hepatitis prevention programs are to screen high-risk persons and to increase the number of infected persons who know their status and are linked to preventive and care services. For communities experiencing health disparities, culturally appropriate education programs can increase awareness of this silent epidemic, and of the health benefits and vaccination and screening, while addressing issues of stigma. Provider education can increase understanding of screening and vaccination policies, interpretation of laboratory tests, and management of viral hepatitis care and treatment. Viral hepatitis services can be integrated with other appropriate prevention services for HIV, STD, and cancer. Public health surveillance and case management can link communities with viral hepatitis prevention and care services.
HHS also recognizes the important health benefits of eliminating HBV transmission. State and local perinatal prevention have a proven track record of success and can provide the necessary services to eliminate HBV among newborns in this country. Studies have shown that cost is a major barrier to successful implementation of adult immunization strategies. Health reform provides new opportunities to increase uptake of immunizations recommended by the HHS Advisory Committee on Immunization Practices (ACIP).
More interventions are needed to prevent hepatitis C. Efforts to find an effective vaccine for HCV should be a continued priority. In the meantime, other new hepatitis C prevention tools must be developed, tested and translated into action. One avenue to explore is to refine and adapt HIV prevention strategies for hepatitis C prevention. Hepatitis C testing and counseling to increase awareness of infection status will promote safe behavioral practices. Together, these approaches can substantially reduce transmission among injection drug users. HHS is working to ensure adherence to proper infection control practices are needed to reduce transmission risks in health care settings, including improved oversight and regulatory approaches, development of new technologies, and training for health care professionals. Rapid tests can improve access to screening, and new assays may improve detection of recent hepatitis C infection. Studies of HCV transmission will help form the evidence base for new interventions. Also, studies suggest that, if detected early, many hepatitis C infections can be cleared (i.e., cured) 36.As new and improved therapies are introduced, research should be conducted to guide how best to use them to preserve the health of those infected and prevent transmission.
The HHS interagency working group will also examine ways to improve viral hepatitis surveillance. Effective prevention requires state and local systems that provide consistent and reliable reporting of new infections, rapid detection of disease outbreaks, and identification and referral of persons with chronic infection for appropriate care and treatment. Currently, CDC estimates that about only 10 percent of new cases of viral hepatitis are reported each year. Two-thirds of states report cases of HCV infection, but those that do have large backlogs of uninvestigated cases. 8 As a result, a clear picture of the nature and scope of chronic HCV infections across every State is not available at this time. HHS is working to improve monitoring of viral hepatitis.
Viral Hepatitis Prevention Activities within HHS
Multiple agencies within HHS are working hard to maximize the impact of available resources in responding to the viral hepatitis epidemic and respond to the recommendations of the IOM report.
Centers for Disease Control and Prevention (CDC)
At CDC, the primary responsibility for prevention and control activities rests with the Division of Viral Hepatitis. Those activities are broadly grouped under four programmatic priorities:
1) Reduce illness and death by identifying persons with viral hepatitis early and referring them to care;
2) Eliminate hepatitis B transmission;
3) Develop, test and translate into action tools to decrease the incidence of HCV; and
4) Guide and evaluate prevention efforts by improving the monitoring of viral hepatitis.
To address those priorities, CDC currently supports viral hepatitis coordinators in 49 states and
the District of Columbia. These coordinators are tasked with integrating viral hepatitis services with other public health efforts to reach populations at risk. While funding does not support direct service provision, the coordinators seek whenever possible to leverage available resources and integrate viral hepatitis education, vaccination, and screening with services provided by federally-supported STD and HIV testing and treatment sites, federally qualified health centers supported by the Health Resources and Services Administration, and other programs.
In addition to supporting coordinators, CDC assists states in responding to disease outbreaks by deploying field investigators and by conducting rapid laboratory serologic and genetic testing to identify sources of infection and direct control strategies. CDC also provides technical support to all states for monitoring acute and chronic infections, including assisting states in adopting surveillance for chronic HBV and HCV infections and investigating cases suggestive of the emergence of rare or new causes of viral hepatitis. Funding for enhanced surveillance activities is provided to 9 state and local health departments.
CDC’s surveillance activities also include monitoring liver cancer incidence and prevalence through the National Program of Cancer Registries, in collaboration with the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program. Data indicate that liver cancer incidence rates vary widely across states, and persistent racial and ethnic disparities exist. 21 These surveillance efforts articulate the burden of liver cancer and can assist states in targeting prevention and control efforts, including primary prevention efforts targeted to the populations most at risk of contracting HBV and HCV.
To identify and address health disparities, CDC surveys populations at increased risk for viral hepatitis, including racial and ethnic minority communities, MSM, and injection drug users. CDC follows approximately 12,000 patients in care for viral hepatitis to study the implementation of recommended preventive and care services.
CDC also supports state and local perinatal prevention coordinators to prevent mother-to-child transmission of hepatitis B. This effort includes ensuring the screening of pregnant women, vaccination of infants at birth, follow-up with infants to ensure completion of the vaccine series, and testing of infants to ensure the development of antibodies. Similarly, through immunization funding for its Adult Hepatitis B Vaccination Initiative, CDC has begun to close the gap in vaccination of at risk adults. Since the beginning of the Initiative in FY 2007, CDC has made approximately $42 million in Section 317 funds available for the purchase of hepatitis B vaccine for use in over 2,600 venues.
Healthcare-associated transmission of viral hepatitis is entirely preventable through adherence to basic infection control. In the area of healthcare-associated transmission of hepatitis, CDC monitors the size and scope of the problem and assists state and local health departments with healthcare-associated outbreak investigations. Perhaps most importantly, CDC identifies best practices regarding infection control and educates providers, patients and industry about these practices through evidence-based infection control guidelines, peer-reviewed publications, and educational campaigns.
In addition to CDC’s work with the states, CDC conducts prevention research to guide policy and program development. CDC fosters development of new approaches to health education, investigation of new screening tests and strategies, studies of licensed and experimental vaccines, and the emergence and implications of viral mutations for diagnosis, prevention, and therapy.
Finally, CDC works with the World Health Organization and other partners to prevent viral hepatitis globally. As of 2008, a total of 177 countries had incorporated hepatitis B vaccine in their national infant immunization programs, and an estimated 69% of the 2008 birth cohort received hepatitis B vaccine. Worldwide, only about 27% of newborns received the birth dose of hepatitis B vaccine.37The FY 2011 Budget includes an increase of 10 percent over the FY 2010 Omnibus to support these activities.
National Institutes of Health (NIH)
At NIH, the primary responsibility for hepatitis research and prevention activities rests with the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and the National Institute of Allergy and Infectious Diseases (NIAID). NIDDK and NIAID support many activities in hepatitis B and C research and education including the following:
Hepatitis B Research: NIAID supports basic and translational research on hepatitis B. Efforts include drug discovery and development and vaccine improvements, as well as many efforts related to HBV pathogenesis and the varying human responses to infection. In addition, the Institute supports many resources for outside investigators to screen and develop new HBV-specific therapeutic candidates at no cost. NIAID resources include tissue culture and animal model screens and preclinical drug development services. In addition, NIAID is currently soliciting applications for research on new classes of HBV therapies.
Hepatitis B Research Network: This multi-center research Network, established in 2008, aims to advance understanding of disease processes and natural history, as well as to develop effective approaches to treating and controlling hepatitis B. The Network currently includes 21 clinical sites across the United States, including Hawaii, and a central data coordinating center. The Network’s centers are in the final stages of planning multiple clinical trials in both adults and children that are responsive to the recommendations of the IOM report regarding pregnant women and at-risk populations.
Clinical Research on Hepatitis C: NIH conducts many clinical trials of available antiviral therapies against hepatitis C, such as the drug interferon. Research to develop a vaccine against hepatitis C is also a major priority for the NIH. Basic and applied studies on hepatitis C virus vaccine development are being funded by NIAID, NIDDK, the National Cancer Institute, and the National Institute on Drug Abuse, including those being conducted by the NIDDK intramural NIDDK Liver Diseases Branch and NIAID’s Laboratory of Infectious Diseases.
Basic Research on Hepatitis C Virus Infection: NIAID and the NIDDK Liver Diseases Branch conduct basic research and fund research on how the hepatitis C virus infects human cells. New animal models and cell culture systems developed by NIAID and NIDDK-funded investigators are instrumental to advancing hepatitis C prevention and therapy. For example, high-impact research projects are developing a mouse model of hepatitis C virus infection and pioneering advanced tissue culture systems that mimic human liver biology for studying the viral life cycle testing new antiviral agents, and identifying viral and human host factors that may serve as targets for future therapies.
The NIAID-supported Hepatitis C Cooperative Research Centers seek to improve basic understanding of HCV pathology. This program, renewed in Fiscal Year (FY) 2010, sponsors five centers which will advance understanding of the host immune response to infection and the factors that determine whether HCV infections are cleared or persist chronically. The underlying mission of the Centers is to help define successful immune response to HCV and identify new targets for drugs, vaccines, and other therapeutic strategies for the prevention or treatment of HCV infection.
NIAID intramural scientists and grantees pursue basic and translational studies on the pathogenesis and molecular biology of HCV, investigate the basic immunology of HCV infection, and partner with industry to further the development of HCV vaccines. NIAID scientists also are collaborating with international researchers to understand why cirrhosis is a fairly stable disease for decades in some patients, while in others it may lead to liver-related death or liver cancer. Investigators are performing genetic analyses and searching for biomarkers for the early detection of liver cancer.
NIAID currently is developing and evaluating new agents to treat HCV/HIV co-infected individuals and is supporting clinical research to define the most effective, long-term treatment strategies for HIV/HCV co-infecton. Currently, NIAID researchers are conducting several clinical studies of patients with chronic viral hepatitis at the NIH Clinical Center. These studies are focused on developing better therapeutics for the management of HCV infection in HIV co-infected individuals.
Trans-NIH and Trans-Agency Viral Hepatitis Research Planning: Strategic research plans, such as the trans-NIH Action Plan for Liver Disease Research, and the National Commission on Digestive Diseases’ research plan, both developed with trans-NIH and trans-HHS input, highlight important research goals relevant to controlling hepatitis B and C. These plans (available at http://liverplan.niddk.nih.gov and http://NCDD.niddk.nih.gov) are currently being implemented by the NIH and partners in the larger research community.
NIH Consensus Development Conferences and Meetings: The NIDDK has provided leadership, along with other NIH Institutes, Centers, and Offices, and other professional organizations, for convening several consensus development conferences on hepatitis B and C, including Management of Hepatitis C (2002), and Management of Hepatitis B (2008). The NIDDK also helped to organize a meeting on Management of Chronic Hepatitis B in 2006, as well as the International Symposium on Viral Hepatitis and Liver Disease in 2009. Recommendations from these conferences and meetings helped to inform the IOM’s report.
Health Resources and Services Administration (HRSA)
Within HRSA, many of the activities related to Hepatitis B and C are overseen by the HIV/AIDS Bureau (HAB) and the Bureau of Primary Health Care (BPHC). HAB and BPHC are collaborating on ways to increase screening and referral to treatment for Federally Qualified Health Center (FQHC) patients who are mono-infected with hepatitis C and those who are dually infected with HIV and hepatitis. Examples of HAB and BPHC hepatitis B and C activities include the following”:
* HRSA/BPHC is working with the Association of Asian Pacific Community Health Organizations (AAPCHO) and the White House Initiative on Asian American and Pacific Islanders to develop strategies for improving prevention and treatment of viral hepatitis among Asian and Pacific Islander Americans.
* Hepatitis C Treatment Expansion Initiative - Evaluation and Technical Assistance Center (CFDA: 93.928): Under the Special Projects of National Significance Program of the
* Ryan White HIV/AIDS program, administered by HRSA’s HIV/AIDS Bureau, this initiative will provide funds for up to 2 years to build capacity among Ryan White-funded
* organizations through the implementation of demonstration models for enhancing HCV treatment protocols in integrated HIV medical treatment settings in the context of providing HIV primary medical care and treatment to individuals co-infected with HCV. In addition to treatment implementation, awarded organizations will also assist the Evaluation and Technical Assistance Center in assessing the effectiveness, feasibility and costs of these service delivery models.
* HRSA supports FQHC services for viral hepatitis treatment and prevention in the following ways:
o Requiring that, as a condition of health center funding and the FQHC "Look-Alike" designation, all federally-funded health centers and FQHC Look-Alikes provide diagnostic lab services, screenings for communicable diseases, and immunizations against vaccine-preventable diseases, including HBV.
o Requiring that federally-funded health centers and FQHC Look-Alikes provide health education to patients and the general community. This includes patient education on diseases that may be prevalent in the community or for which the population may be vulnerable, such as viral hepatitis.
o HRSA promotes screening and treatment of viral hepatitis through a national cooperative agreement. Activities resulting from this agreement include raising awareness of viral hepatitis among health center providers and patients, and providing technical assistance on strategies to treat and prevent viral hepatitis. For example, HRSA recently met with the National Alliance of State and Territorial AIDS Directors and the Northeast Hepatitis Coordinators’ Alliance to strategize on hepatitis prevention and treatment in FQHCs.
* In order to better monitor hepatitis incidence in health center patients, HRSA revised its health center grantee reporting mechanism to track patient hepatitis rates.
* The only successful treatment available for endstage liver disease due to HCV is liver transplantation. HRSA provides oversight for the Organ Procurement and Transplantation Network (OPTN) operated under contract by United Network for Organ Sharing (UNOS). Currently there are 16,072 patients on the nationwide liver transplant waiting list, and 6.320 liver transplants were performed in 2009. Because of the critical shortage of donor organs, 1,461 patients died in 2009 waiting for a liver transplant. About 40% of liver transplants performed in the U.S. have HCV, and experts expect this number to rise significantly during the next decade. Although liver transplantation can successfully treat chronic liver failure due to HCV, a major challenge facing these recipients is recurrence of HCV in the new liver that eventually leads to reduced graft survival. 38
Food and Drug Administration (FDA)
The FDA has multiple centers working on hepatitis B and C prevention activities:
CDER Activities Relating to Hepatitis B and C: FDA’s Center for Drug Evaluation and Research (CDER) has the responsibility of reviewing drug products and certain biological products including therapeutic proteins and monoclonal antibodies for the treatment and/or prevention of viral hepatitis including hepatitis B and C.
Currently, there is a great deal of interest within industry in developing treatments for both hepatitis B and C. FDA has approved five drugs and two interferon products to treat hepatitis B. FDA has approved three distinct types of interferon products from three different sponsors for the treatment of hepatitis C. FDA has also approved multiple versions of ribavirin, a drug approved to increase the effectiveness of intereferons in the treatment of hepatits C.
CDER also regularly meets with numerous issue groups and pharmaceutical companies to discuss drug development plans, protocols and proposals. CDER is currently collaborating with the Forum for HIV Research to plan a workshop on hepatitis C drug development. FDA also held a public meeting in April 2010 to discuss expanded access to direct-acting antiviral agents for the treatment of chronic hepatitis C infection in patients with unmet medical need. CDER is in the process of drafting a guidance to industry on the development of direct-acting antivirals for the treatment of hepatitis C. And lastly, FDA issued a Citizen Petition response which recognized the crisis of hepatitis C among people with bleeding disorders and the need to take definite steps to allow people with bleeding disorders and hepatitis C and other patients with hepatitis C with no treatment options to have access to promising investigational drugs beyond current clinical trials.
CBER Activities Relating to Hepatitis B and C: The FDA’s Center for Biologics Evaluation and Research (CBER) regulates biological products for human use under applicable federal laws, including the Public Health Service Act and the Federal Food, Drug, and Cosmetic Act. CBER protects and promotes the public health by ensuring that biological products are safe and effective and available to those who need them. CBER also provides the public with information to promote the safe and appropriate use of biological products. CBER regulates an array of diverse and complex biological products, both investigational and licensed, including vaccines, blood and blood products, and human tissues and cellular products. In carrying out its mission to ensure the safety, purity, and potency (effectiveness) of biological products, CBER engages in a number of activities pertinent to HBV and HCV.
Scientists in CBER laboratories are currently working on several research projects pertaining to HCV. One research program, Hepatitis C Vaccines: Development of in vitro and in vivo Systems for HCV Replication and Evaluation of Vaccine Efficacy, seeks to evaluate new methods and models for evaluating the immune responses to HCV in systems that may be predictive of outcomes in people. Evaluating immune correlates of protection will be invaluable in the assessment of candidate HCV vaccines and to support development of new HCV vaccines.
Another research program – Studies of Efficacy, Safety and Potency Assay Development for Prophylactic and Therapeutic Vaccines against Hepatitis Viruses – is focused on developing scientific tools to understand the immunobiology and pathogenesis of HCV. Studies include the development of a small animal model for HCV infection, identification of efficacy biomarkers (i.e., immunologic correlates of protection), development of neutralization tests for the virus, use of nanotechnology for induction of protective immune responses, and studies on the safety of therapeutic vaccines for this virus. These studies will provide the ability to evaluate new technologies being applied to vaccine development, and will be pivotal in guiding and assessing the safety, efficacy and manufacturing issues associated with HCV vaccines.
CBER also engages in research activities pertaining to the safety and efficacy of plasma-derived products in the context of HBV and HCV. CBER research studies have impacted: (1) the safety of blood and blood products with respect to viral pathogens in transfusion recipients; (2) the establishment of national, international, or global standards that would ensure the safety of blood and potency of plasma-derived products; and (3) the development of cell culture based-assays to test for pathogen inactivation.
CDRH Activities Relating to Hepatitis B and C: FDA's Center for Devices and Radiological Health (CDRH), which is responsible for regulating firms who manufacture, repackage, relabel, and/or import medical devices sold in the United States, has a dedicated Office of In Vitro Diagnostic Device Evaluation and Safety (OIVD) charged with regulating all aspects of in-home and laboratory diagnostic tests (in vitro diagnostic devices, or IVDs). OIVD's multidisciplinary group of scientists, medical technologists, policy analysts, engineers, pathologists, and clinicians has a dual charge to foster the rapid transfer of new IVDs into the marketplace while preventing marketing of unsafe or ineffective devices, and is engaged in a number of activities related to hepatitis B and hepatitis C.
In addition, OIVD scientific reviewers and managers participate in several interagency groups associated with viral liver disease. The Hepatitis "Think C" Personalized Medicine Group works to improve the dosage of anti-viral medication at the individual patient level through a combination of appropriate diagnostic test and drug regimes. The Liver Fibrosis Interagency Group meets to discuss the ongoing search for new diagnostic biomarkers for liver fibrosis, which could replace the current practice of diagnosis by liver biopsy.
Indian Health Service (IHS)
IHS works to prevent viral hepatitis in its beneficiary population. IHS has a vaccination program to prevent hepatitis B in the Indian communities it serves. Routine vaccination of all newborns occurs at IHS birthing hospitals, with the first dose of hepatitis B vaccine administered as soon as possible after birth. The hepatitis B vaccine series started at birth is completed as part of normal pediatric vaccine schedule. Catch-up hepatitis B vaccination is offered to children and adolescents who need it. Vaccination of at-risk adults varies by site. Screening for the hepatitis B surface antigen in pregnant IHS patients is generally done as part of the regular health care treatment protocol. Treatment of chronic hepatitis B is provided, most notably in Alaska.
Treatment of hepatitis C occurs at some service units, with four IHS areas providing hepatitis C treatment in at least one service unit. Again, the Alaska Area offers the most developed program. The Seattle Indian Health Board Viral Hepatitis Education and Training (VHET) Project offers education and training of providers in screening of at-risk adults for hepatitis B and hepatitis C, and in hepatitis A and B vaccination. The IHS is also developing electronic health record-based surveillance methods to describe the epidemiology of hepatitis C in the HIS beneficiary population.
HHS Office of Minority Health (OMH)
OMH helped sponsor the IOM report, and is ingworking to elevate viral hepatitis as a priority public health issue. AActivities led by OMH include the following:
Hepatitis B Video, titled “B”/PSA: The OMH was asked by the Association of Asian Pacific Community Health Organizations and the Hepatitis B Foundation to collaborate on the national release of the Hepatitis “B” video/PSA. The PSA was awarded the Grand Prize of the B Real Short Film Competition at the Los Angeles Asian Pacific Film Festival in 2009 and, prior to the partnership with OMH, was played in every major feature at the Asian American International Film Festival in New York. As part of the partnership, the PSA was recently aired on ABC during the Oprah Winfrey Show, CNN’s Anderson Cooper, Good Morning America, Today Show, the evening news and various Asian media networks. The PSA will be translated into six different Asian languages.
World Hepatitis Day: The OMH, Association of Asian Pacific Community Health Organizations, National Alliance of State and Territorial AIDS Directors, and National Viral Hepatitis Roundtable recently hosted a World Hepatitis Day event to highlight the importance of global action to eliminate viral hepatitis in Asian American, Native Hawaiian, Pacific Islander, African American, American Indian, Alaska Native, and Hispanic/Latino communities.
Compendium Distribution: Compendium on Local Hepatitis B Activities: The Association of Asian Pacific Community Health Organizations (AAPCHO) received an OMH National Umbrella Cooperative Agreement to enhance hepatitis B activities in communities across the nation. As part of this award, AAPCHO will work with the Hepatitis B Foundation and Asian Pacific Islander American Health Forum to develop and implement a comprehensive strategy to promote and distribute a hepatitis B compendium to catalyze partnerships for local and national action.
The compendium includes case studies on the successes and lessons learned from local coalitions that are part of AAPCHO's hepatitis "B Activated" network. The case studies provide examples and recommendations for enhancing coalition efforts for increasing local awareness, and enhancing screening and vaccination activities. The compendium is intended for communities who are interested in developing or strengthening local hepatitis B awareness and prevention efforts.
Bilingual Bicultural Demonstration Program: Funded by OMH under the Bilingual Bicultural Demonstration Program, the Asian Liver Center at Stanford University’s “Building the Community Partnership for San Francisco: Hep B Free Campaign” works to screen, vaccinate and treat all San Francisco Asian and Pacific Islander residents against hepatitis B by providing convenient, free or low-cost testing opportunities at partnering health facilities.
Community Partnership: The Immigrant and Refugee Community Organization (IRCO), an OMH Community Partnership grantee, seeks to decrease the prevalence of hepatitis B and HIV in the Asian and Pacific Islander, African Refugee, and Immigrant communities in Portland, Oregon. Since September 2009, IRCO has reached 210 members of the Asian and African refugee and immigrant community and trained 43 healthcare interpreters on hepatitis B transmission, symptoms, and the importance of early detection.
Closing
Given the substantial and increasing disease and economic burden from viral hepatitis, HHS is taking immediate and coordinated steps to reverse these trends, which represent a health priority for our nation. HHS greatly appreciates the committee’s interest in these important issues.
Thank you for the opportunity to share this information with you. I recognize that the problems I have identified are significant ones, but I am confident that working together we can succeed in protecting this nation against the needless disease, pain, suffering, and death caused by viral hepatitis. Thank you. I will be happy to answer any questions.
1 Goldstein ST, Zhou F, Hadler SC, Bell BP, Mast EE, Margolis HS. A mathematical model to estimate global hepatitis B disease burden and vaccination impact. Int J Epidemiol 2005;34:1329--39
2 World Health Organization. Hepatitis B. Geneva, Switzerland: World Health Organization; 2000. Available at http://www.who.int/mediacentre/factsheets/fs204/en/print.html
3 W.M. Lee, Hepatitis B virus infection, N Engl J Med 337 (1997) (24), pp. 1733–1745.
4 Perz, J.F., The contribution of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. Journal of Hepatology 2006; 45 (4):529-538.
5 WHO Cancer Fact Sheet No 297 Feb 2009. http://www.who.int/mediacentre/factsheets/fs297/en/print.html
6 CDC. Hepatocellular carcinoma – United States, 2001-2006. MMWR 2010;59 (17:517-20).
7 IOM (Institute of Medicine). Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: The National Academies Press. At 21 (2010)
8 Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med 2006;144:705--14
9 CDC. Surveillance for Acute Viral Hepatitis – United States, 2007. 2009;58 (No. SS-3)
10 CDC. Recommendations for Identification and Public Health Management of Persons with Chronic Hepatitis B Virus Infection. 2008;57 (No. RR-8)
11 Lok AS, McMahon BJ. Chronic Hepatitis B. Hepatology2007; 45:507-539
12 Seeff LB. Natural History of Chronic Hepatitis C. Hepatology 2002; 36:S35-S46.
13 Brown RS Jr. Hepatitis C and liver transplantation. Nature 2005;436:973-978.
14 Sherman KE, Rouster SD, Chung RT, Rajicic N. Hepatitis C virus prevalence among patients coinfected with human immunodeficiency virus: a cross-sectional analysis of the U.S. Adult AIDS Clinical Trials Group. Clin Infect Dis 2002;34:831-7.
15 D:A:D Study Group. Factors associated with specific causes of death amongst HIV-positive individuals in the D:A:D study. AIDS 2010 [epublication May 6, 2010 ahead of print]
16 Altekruse SF, McGlynn KA, Reichman ME. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol 2009;27:1485--91.
17Vogt T, Wise ME, Shih H, Williams IT. Hepatitis B Mortality in the United States, 1990-2004 [Abstract]. 45th Annual Meeting of Infectious Diseases Society of America, San Diego, CA; October 4-7, 2007
18 Wise M et al. Changing trends in hepatitis C-related mortality in the United States, 1995–2004. Hepatology 2008;47:1–8.
19 CDC. Screening for Chronic Hepatitis B Among Asian/Pacific Islander Populations – New York City, 2005. MMWR 2006; 55(18):505-509.
20 CDC. Hepatocellular carcinoma – United States, 2001-2006. MMWR 2010;59(17;517-20.
21 Edmunds WJ, Medley GF, Nokes DJ, Hall AJ, Whittle HC. The influence of age on the development of the hepatitis B carrier state. Proc R Soc Lond B Biol Sci 1993;253:197--201
22 McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 1985;151:599--603.
23 Hyams KC. Risks of chronicity following acute hepatitis B virus infection: a review. Clin Infect Dis 1995;20:992--1000
24 CDC. Hepatitis B Virus: A Comprehensive Strategy for Eliminating Transmission in the United States Through Universal Childhood Vaccination: Recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR 1991;40 (RR-13): 1-19. http://www.cdc.gov/mmwr/preview/mmwrhtml/00033405.htm
25 Estimated Vaccination Coverage* with Individual Vaccines and Selected Vaccination Series Among Children 19-35 Months of Age by State and Local Area US, National Immunization Survey, Q1/2008-Q4/2008† http://www2a.cdc.gov/nip/coverage/nis/nis_iap2.asp?fmt=v&rpt=tab02_antigen_iap&qtr=Q1/2008-Q4/2008
26 CDC. National, State, and Local Area Vaccination Coverage Among Children Aged 19--35 Months --- United States, 2008. MMWR 2009;58: 921-926.
27 CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: immunization of infants, children, and adolescents. MMWR 2005;54 (RR-16):1–31.
28 CDC Unpublished Data
29 JB Wong, GM McQuillan, JG McHutchison and T Poynard. Estimating future hepatitis C morbidity, mortality, and costs in the United States, American Journal of Public Health, Vol 90, Issue 10 1562-1569.
30 Milliman Study for Vertex Pharmaceuticals. Consequences of Hepatitis C Virus – Costs of a Baby Boomer Epidemic of Liver Disease. 2009
31 A Rajendra, JB Wong Economics of chronic hepatitis B and hepatitis C Journal of Hepatology, 2007 Oct: 47 (4):608-17. Epub 2007 Jul 30
32 Kanwal F, et al., Treatment alternatives for hepatitis B cirrhosis: a cost-effectiveness analysis. The American Journal of Gastroenterology, 2006;101(9):2067-2089.
33 Spackman DE, Veenstra D. A cost-effectiveness analysis of currently approved treatments for HBeAg-positive chronic hepatitis B. PharmacoEconomics, 2008;26(11):937-949.
34 Wong JB, et al., Cost-effectiveness of interferon-alpha 2b treatment for hepatitis B e antigen-positive chronic hepatitis B. Ann Intern Med, 1995;122(9):664-675
35 Hutton DW, Tan D, So SK, et al. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med, 2007;147(7):460-469.
36 Licata A, DiBona D, Schepis F, Shahied L, Craxi A, Camma C. When and How to Treat Acute Hepatitis C? J Hepatol 2003;39:1056-1062
37 CDC. Implementation of Newborn Hepatitis B Vaccination – Worldwide, 2006. MMWR 2008;57(46):1249-1252.
38 TD Schiano and P Martin, Review: Management of HCV infection and liver transplantation, International Journal of Medical Sciences (2006) 3(2):79-83.
Last revised: September 09,2010
Statement by Howard K Koh, M.D., M.P.H.,
Assistant Secretary for Health
U.S. Department of Health and Human Services (HHS)
on
Viral Hepatitis: The Secret Epidemic
before
Committee on Oversight and Governmental Reform
United States House of Representatives
Thursday, June 17, 2010
Good morning, Chairman Towns, Ranking Member Issa, and other distinguished Members of the Committee. I am Dr. Howard Koh, the Assistant Secretary for Health in the Department of Health and Human Services (HHS or the Department). I am honored to be here today to discuss the silent epidemic of viral hepatitis in this country, and the coordinated steps the Department is taking to effectively address this significant public health problem through better prevention, care and monitoring efforts.
Viral hepatitis is a collective term describing liver inflammation or hepatitis caused by a group of several different viruses. Three viruses, Hepatitis A virus (HAV), Hepatitis B virus (HBV) and Hepatitis C virus (HCV) cause most viral hepatitis in the United States. Spread in unsanitary conditions, hepatitis A cases have declined significantly in the U.S. in recent years as a result of vaccination programs and food safety efforts. Today, I will focus my remarks on the prevention of HBV and HCV transmission and associated morbidity and mortality. Unlike HAV, HBV and HCV infections are blood-borne and often persist for years, resulting in ongoing (chronic) but usually asymptomatic liver inflammation, and in some cases scarring (cirrhosis) that leads to liver failure and/or and liver cancer. Chronic hepatitis is a major cause of liver cancer and chronic liver disease globally and in the United States.
HBV and HCV Disease Burden
Worldwide, 480 million to 540 million persons are living with chronic viral hepatitis, with 350 million 1, 2 to 370 3 million infected with HBV and 130 million to 170 million infected with HCV.4
All told, chronic viral hepatitis afflicts about 1 in every 12 persons worldwide. About 54,000 persons with chronic hepatitis B infections immigrate to the U.S. annually. Chronic hepatitis causes considerable morbidity. Globally, an estimated 78% of primary liver cancer and 57% of liver cirrhosis are caused by chronic viral hepatitis and about one million deaths from viral hepatitis occur each year.4 Liver cancer is the fourth -leading cause of death from cancer worldwide, the third -leading cause among men.5 The most recent liver cancer surveillance data indicate that long-term liver cancer incidence is increasing in the U.S., with an average annual percentage change in incidence between 2001 and 2006 of 3.5% per year.6
In the United States, viral hepatitis remains no less of a problem; 3.5 million to 5.3 million Americans have chronic viral hepatitis. 7, 8, 9 The vast majority, an estimated 65 % and 75% are not aware they are infected with HBV and HCV, respectively. 7 In the absence of appropriate treatment, 15-40% of infected persons will develop liver cirrhosis. 10, 11, 12 Viral hepatitis is the leading cause of liver transplantation in the United States. 13 Co-factors, including HIV, excessive alcohol use, and fatty liver disease associated with obesity and diabetes, amplify the effects of viral hepatitis, hastening development of liver disease. Fifteen to thirty percent of all persons infected with HIV have chronic viral hepatitis, 14 and liver disease is now the main non-AIDS cause of death in HIV-infected persons. 15 In contrast to almost all other types of cancer, liver cancer rates have tripled over the last several decades, 16 fueled in large part by the progression of viral hepatitis to end-stage disease among persons infected years ago. In the United States, viral hepatitis causes 12,000 to 15,000 deaths annually, 17, 18 and viral hepatitis-related illness, deaths, and costs are all expected to rise substantially in the coming years.
Viral hepatitis poses a major health threat for certain populations. Among persons aged 46 to 64 years (i.e., baby boomers), about 1 in 33 have chronic viral hepatitis. 9 One out of every 7 African American men in their 40s is living with chronic hepatitis C, 9 and approximately 1 in 12 Asian Americans is living with chronic hepatitis B. 19 Similarly, the profiles of persons with liver cancer mirror the demographic characteristics of persons with chronic viral hepatitis; liver cancer incidence is highest among Asians/Pacific Islanders, and is increasing among Hispanics, African Americans, baby boomers, and males. 20
New HBV and HCV infections add to the burden of chronic viral hepatitis and liver disease. In 2007, there were an estimated 43,000 new cases of HBV infection. 10 HBV is spread from mother to child at the time of birth, among household contacts through incidental blood exposures in the home, through injection drug use, and through sexual contact. Viral hepatitis transmission should never occur as a result of health care delivery, but transmission has been documented in a variety of health care settings when providers have failed to follow basic infection control practices. Rates of HBV infection are highest among adults, reflecting low hepatitis B vaccination coverage among persons with risks such as injection drug use and multiple sexual partners. Prevention of mother-to-child transmission is critical, as 90% of HBV -infected newborns remain infected 21, 22, 23 and about 1 in 4 die from complications of chronic viral hepatitis in later life. 11 Outbreaks of hepatitis B occur in persons not currently recommended to receive the vaccine, such as persons with diabetes, patients in outpatient settings, and residents of long term care facilities; they also occur in health care settings when providers fail to follow basic infection control.
Surveillance data suggest nearly 20,000 10 persons are newly infected with HCV annually in the United States. HCV is primarily a blood-borne virus spread through injection drug use. Transmission also occurs in health care settings as a result of unacceptable lapses in infection control, primarily related to the misuse of syringes and medication vials. Non-injecting drug users who snort cocaine and other drugs also have elevated risks for HCV, possibly from blood exposure associated with intranasal use. Perhaps typically thought of as an urban disease, HCV transmission has been detected among young drug users in suburban and rural communities. In addition, after reports from Europe for several years, sexual transmission of HCV has been detected among U.S. cohorts of HIV-infected men who have sex with men (MSM). In certain circumstances, HCV can be transmitted sexually and at the time of birth.
Public Health Prevention Measures to Address Viral Hepatitis
Public health measures can prevent transmission. These measures have helped our nation achieve remarkable declines in the number of new infections with both viruses. Safe and effective vaccines are available to provide long term protection from hepatitis B. In 1991, the Centers for Disease Control and Prevention (CDC) and the national Advisory Committee on Immunization Practices (ACIP) set forth an ambitious vaccine-based strategy to eliminate HBV transmission in the United States. 24 This strategy involves vaccinating newborns and older children, as well as vaccinating at-risk adults.
Routine vaccination of infants and catch-up vaccination of older children under federally -supported vaccination programs has successfully driven down rates of HBV transmission and acute cases of disease, with rates falling 82% from 8.5 cases per 100,000 population in 1990 to 1.5 cases per 100,000 population in 2007, the most recent year for which data are available. 10 Rates have declined most dramatically—98%—among children aged 15 years and younger. Vaccine coverage among children aged 19 months to 35 months is 93%. 25, 26
In the United States, approximately 24,000 HBV-infected women give birth each year 27 , most of whom are identified by prenatal screening. Their infants are recommended to receive protective hepatitis B vaccination and other prevention services. State and local prevention programs currently do not have the capacity to manage all of the estimated newborns who are exposed. To assure newborns exposed to HBV are protected, CDC recommends that all infants receive a birth dose of hepatitis B vaccine. In 2008, 55% of newborns received a birth dose in the first three days of life. 30 As not all newborns receive protective interventions, each year hundreds of infants are infected with HBV in the United States. 28
Hepatitis B vaccine is also recommended for adults with sexual and blood exposure risks. As the result of improvements in infection control and ongoing hepatitis B vaccination, relatively few cases now occur in certain populations such as dialysis patients and healthcare workers that previously were considered to be at high risk. However, while the number of new cases has declined among adults, 95 % of all new cases are among adults. A high proportion of those cases occur among persons with risk behaviors such as injecting drug users, MSM, and persons with multiple sex partners. Rates are particularly high among males aged 25 to 44 years old. 10
Unlike HBV, there is no vaccine yet developed for HCV. However, since HCV was discovered in the 1980s, the development of prevention interventions has caused a significant decline in new cases. Screening of donated blood and other tissues and organs now protects recipients of these donations. Screening, together with behavioral education, and access to clean syringes and drug treatment have had a role in reducing the number of new cases of HCV related to injection drug use 8 In addition, the adoption of standard precautions in health care settings has reduced transmission risks for all blood -borne viruses, including HBV and HCV.
The onset of liver cancer and other liver disease can be prevented through screening and care for persons chronically infected with HBV or HCV. Current treatments can halt or even reverse the liver damage caused by viral hepatitis. New treatments on the immediate horizon hold even greater promise for a definitive cure. CDC recommends screening to identify persons with viral hepatitis and prevention and care services to reduce transmission and morbidity.
Prevention and care for viral hepatitis makes economic sense. Published studies estimate that medical costs for viral hepatitis run in the billions of dollars per year. 29, 30 Numerous studies reveal the cost-effective benefits of screening and care for populations at risk for viral hepatitis. 31, 32, 33, 34 Hepatitis screening linked to vaccination and care is a cost -effective prevention approach to eliminating health disparities for Asian and Pacific Island Americans. 35 Preliminary data from a CDC model show that by identifying and referring for appropriate care all HCV-infected persons in primary care, approximately 87,000 cases of end stage liver disease and 11,000 liver transplants can be prevented, and 840,000 undiscounted life years would be gained, with an estimated cost per discounted quality adjusted life year, or QALY, of $43,000. Similarly, preliminary estimates reveal that expanded HBV screening and care could avert approximately 140,000 cases of end stage liver disease and gain 3.3 million QALYs.
The Institute of Medicine Report
In January 2010, The Institute of Medicine (IOM) issued a report titled, Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. The report identified multiple barriers that have combined to create a situation in which inadequate public resources are available to support the prevention, care and monitoring needed to fully and effectively address this important public health problem.
The IOM report described deficiencies that have created adverse consequences for the health of our nation:
* Inadequate disease surveillance systems underreport acute and chronic infections, so the full extent of the problem is unknown;
* At-risk people do not know that they are at risk or how to prevent becoming infected;
* At-risk people may not have access to prevention services;
* Chronically infected people do not know they are infected;
* Many healthcare providers do not screen people for risk factors or do not know how to manage infected people; and
* Infected people often have inadequate access to testing, social support, and medical management services.
The IOM called for an intensified, coordinated national effort to improve the prevention of viral hepatitis and better protect the health of Americans.
The HHS Response to the IOM Report
HHS and its agencies are fully committed to accelerating progress towards the prevention of viral hepatitis and associated disease in the U.S., and advancing this strategy. In January, HHS established an interagency work group on viral hepatitis, which I chair, that has diverse representation from HHS operating divisions. A work group subcommittee is currently drafting a comprehensive strategic action plan for HHS to improve the coordination of viral hepatitis prevention, care and monitoring activities within the Department. The action plan is grouped by focus areas: Increasing community awareness and provider education; strengthening surveillance for viral hepatitis; preventing viral hepatitis transmission through vaccination; preventing blood-borne transmission; and improving clinical preventive care and treatment services. The current timeline is to complete this action plan by October 1, fall 2010.
There are millions of persons who are unaware they have a potentially life -threatening disease. Major goals of viral hepatitis prevention programs are to screen high-risk persons and to increase the number of infected persons who know their status and are linked to preventive and care services. For communities experiencing health disparities, culturally appropriate education programs can increase awareness of this silent epidemic, and of the health benefits and vaccination and screening, while addressing issues of stigma. Provider education can increase understanding of screening and vaccination policies, interpretation of laboratory tests, and management of viral hepatitis care and treatment. Viral hepatitis services can be integrated with other appropriate prevention services for HIV, STD, and cancer. Public health surveillance and case management can link communities with viral hepatitis prevention and care services.
HHS also recognizes the important health benefits of eliminating HBV transmission. State and local perinatal prevention have a proven track record of success and can provide the necessary services to eliminate HBV among newborns in this country. Studies have shown that cost is a major barrier to successful implementation of adult immunization strategies. Health reform provides new opportunities to increase uptake of immunizations recommended by the HHS Advisory Committee on Immunization Practices (ACIP).
More interventions are needed to prevent hepatitis C. Efforts to find an effective vaccine for HCV should be a continued priority. In the meantime, other new hepatitis C prevention tools must be developed, tested and translated into action. One avenue to explore is to refine and adapt HIV prevention strategies for hepatitis C prevention. Hepatitis C testing and counseling to increase awareness of infection status will promote safe behavioral practices. Together, these approaches can substantially reduce transmission among injection drug users. HHS is working to ensure adherence to proper infection control practices are needed to reduce transmission risks in health care settings, including improved oversight and regulatory approaches, development of new technologies, and training for health care professionals. Rapid tests can improve access to screening, and new assays may improve detection of recent hepatitis C infection. Studies of HCV transmission will help form the evidence base for new interventions. Also, studies suggest that, if detected early, many hepatitis C infections can be cleared (i.e., cured) 36.As new and improved therapies are introduced, research should be conducted to guide how best to use them to preserve the health of those infected and prevent transmission.
The HHS interagency working group will also examine ways to improve viral hepatitis surveillance. Effective prevention requires state and local systems that provide consistent and reliable reporting of new infections, rapid detection of disease outbreaks, and identification and referral of persons with chronic infection for appropriate care and treatment. Currently, CDC estimates that about only 10 percent of new cases of viral hepatitis are reported each year. Two-thirds of states report cases of HCV infection, but those that do have large backlogs of uninvestigated cases. 8 As a result, a clear picture of the nature and scope of chronic HCV infections across every State is not available at this time. HHS is working to improve monitoring of viral hepatitis.
Viral Hepatitis Prevention Activities within HHS
Multiple agencies within HHS are working hard to maximize the impact of available resources in responding to the viral hepatitis epidemic and respond to the recommendations of the IOM report.
Centers for Disease Control and Prevention (CDC)
At CDC, the primary responsibility for prevention and control activities rests with the Division of Viral Hepatitis. Those activities are broadly grouped under four programmatic priorities:
1) Reduce illness and death by identifying persons with viral hepatitis early and referring them to care;
2) Eliminate hepatitis B transmission;
3) Develop, test and translate into action tools to decrease the incidence of HCV; and
4) Guide and evaluate prevention efforts by improving the monitoring of viral hepatitis.
To address those priorities, CDC currently supports viral hepatitis coordinators in 49 states and
the District of Columbia. These coordinators are tasked with integrating viral hepatitis services with other public health efforts to reach populations at risk. While funding does not support direct service provision, the coordinators seek whenever possible to leverage available resources and integrate viral hepatitis education, vaccination, and screening with services provided by federally-supported STD and HIV testing and treatment sites, federally qualified health centers supported by the Health Resources and Services Administration, and other programs.
In addition to supporting coordinators, CDC assists states in responding to disease outbreaks by deploying field investigators and by conducting rapid laboratory serologic and genetic testing to identify sources of infection and direct control strategies. CDC also provides technical support to all states for monitoring acute and chronic infections, including assisting states in adopting surveillance for chronic HBV and HCV infections and investigating cases suggestive of the emergence of rare or new causes of viral hepatitis. Funding for enhanced surveillance activities is provided to 9 state and local health departments.
CDC’s surveillance activities also include monitoring liver cancer incidence and prevalence through the National Program of Cancer Registries, in collaboration with the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program. Data indicate that liver cancer incidence rates vary widely across states, and persistent racial and ethnic disparities exist. 21 These surveillance efforts articulate the burden of liver cancer and can assist states in targeting prevention and control efforts, including primary prevention efforts targeted to the populations most at risk of contracting HBV and HCV.
To identify and address health disparities, CDC surveys populations at increased risk for viral hepatitis, including racial and ethnic minority communities, MSM, and injection drug users. CDC follows approximately 12,000 patients in care for viral hepatitis to study the implementation of recommended preventive and care services.
CDC also supports state and local perinatal prevention coordinators to prevent mother-to-child transmission of hepatitis B. This effort includes ensuring the screening of pregnant women, vaccination of infants at birth, follow-up with infants to ensure completion of the vaccine series, and testing of infants to ensure the development of antibodies. Similarly, through immunization funding for its Adult Hepatitis B Vaccination Initiative, CDC has begun to close the gap in vaccination of at risk adults. Since the beginning of the Initiative in FY 2007, CDC has made approximately $42 million in Section 317 funds available for the purchase of hepatitis B vaccine for use in over 2,600 venues.
Healthcare-associated transmission of viral hepatitis is entirely preventable through adherence to basic infection control. In the area of healthcare-associated transmission of hepatitis, CDC monitors the size and scope of the problem and assists state and local health departments with healthcare-associated outbreak investigations. Perhaps most importantly, CDC identifies best practices regarding infection control and educates providers, patients and industry about these practices through evidence-based infection control guidelines, peer-reviewed publications, and educational campaigns.
In addition to CDC’s work with the states, CDC conducts prevention research to guide policy and program development. CDC fosters development of new approaches to health education, investigation of new screening tests and strategies, studies of licensed and experimental vaccines, and the emergence and implications of viral mutations for diagnosis, prevention, and therapy.
Finally, CDC works with the World Health Organization and other partners to prevent viral hepatitis globally. As of 2008, a total of 177 countries had incorporated hepatitis B vaccine in their national infant immunization programs, and an estimated 69% of the 2008 birth cohort received hepatitis B vaccine. Worldwide, only about 27% of newborns received the birth dose of hepatitis B vaccine.37The FY 2011 Budget includes an increase of 10 percent over the FY 2010 Omnibus to support these activities.
National Institutes of Health (NIH)
At NIH, the primary responsibility for hepatitis research and prevention activities rests with the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and the National Institute of Allergy and Infectious Diseases (NIAID). NIDDK and NIAID support many activities in hepatitis B and C research and education including the following:
Hepatitis B Research: NIAID supports basic and translational research on hepatitis B. Efforts include drug discovery and development and vaccine improvements, as well as many efforts related to HBV pathogenesis and the varying human responses to infection. In addition, the Institute supports many resources for outside investigators to screen and develop new HBV-specific therapeutic candidates at no cost. NIAID resources include tissue culture and animal model screens and preclinical drug development services. In addition, NIAID is currently soliciting applications for research on new classes of HBV therapies.
Hepatitis B Research Network: This multi-center research Network, established in 2008, aims to advance understanding of disease processes and natural history, as well as to develop effective approaches to treating and controlling hepatitis B. The Network currently includes 21 clinical sites across the United States, including Hawaii, and a central data coordinating center. The Network’s centers are in the final stages of planning multiple clinical trials in both adults and children that are responsive to the recommendations of the IOM report regarding pregnant women and at-risk populations.
Clinical Research on Hepatitis C: NIH conducts many clinical trials of available antiviral therapies against hepatitis C, such as the drug interferon. Research to develop a vaccine against hepatitis C is also a major priority for the NIH. Basic and applied studies on hepatitis C virus vaccine development are being funded by NIAID, NIDDK, the National Cancer Institute, and the National Institute on Drug Abuse, including those being conducted by the NIDDK intramural NIDDK Liver Diseases Branch and NIAID’s Laboratory of Infectious Diseases.
Basic Research on Hepatitis C Virus Infection: NIAID and the NIDDK Liver Diseases Branch conduct basic research and fund research on how the hepatitis C virus infects human cells. New animal models and cell culture systems developed by NIAID and NIDDK-funded investigators are instrumental to advancing hepatitis C prevention and therapy. For example, high-impact research projects are developing a mouse model of hepatitis C virus infection and pioneering advanced tissue culture systems that mimic human liver biology for studying the viral life cycle testing new antiviral agents, and identifying viral and human host factors that may serve as targets for future therapies.
The NIAID-supported Hepatitis C Cooperative Research Centers seek to improve basic understanding of HCV pathology. This program, renewed in Fiscal Year (FY) 2010, sponsors five centers which will advance understanding of the host immune response to infection and the factors that determine whether HCV infections are cleared or persist chronically. The underlying mission of the Centers is to help define successful immune response to HCV and identify new targets for drugs, vaccines, and other therapeutic strategies for the prevention or treatment of HCV infection.
NIAID intramural scientists and grantees pursue basic and translational studies on the pathogenesis and molecular biology of HCV, investigate the basic immunology of HCV infection, and partner with industry to further the development of HCV vaccines. NIAID scientists also are collaborating with international researchers to understand why cirrhosis is a fairly stable disease for decades in some patients, while in others it may lead to liver-related death or liver cancer. Investigators are performing genetic analyses and searching for biomarkers for the early detection of liver cancer.
NIAID currently is developing and evaluating new agents to treat HCV/HIV co-infected individuals and is supporting clinical research to define the most effective, long-term treatment strategies for HIV/HCV co-infecton. Currently, NIAID researchers are conducting several clinical studies of patients with chronic viral hepatitis at the NIH Clinical Center. These studies are focused on developing better therapeutics for the management of HCV infection in HIV co-infected individuals.
Trans-NIH and Trans-Agency Viral Hepatitis Research Planning: Strategic research plans, such as the trans-NIH Action Plan for Liver Disease Research, and the National Commission on Digestive Diseases’ research plan, both developed with trans-NIH and trans-HHS input, highlight important research goals relevant to controlling hepatitis B and C. These plans (available at http://liverplan.niddk.nih.gov and http://NCDD.niddk.nih.gov) are currently being implemented by the NIH and partners in the larger research community.
NIH Consensus Development Conferences and Meetings: The NIDDK has provided leadership, along with other NIH Institutes, Centers, and Offices, and other professional organizations, for convening several consensus development conferences on hepatitis B and C, including Management of Hepatitis C (2002), and Management of Hepatitis B (2008). The NIDDK also helped to organize a meeting on Management of Chronic Hepatitis B in 2006, as well as the International Symposium on Viral Hepatitis and Liver Disease in 2009. Recommendations from these conferences and meetings helped to inform the IOM’s report.
Health Resources and Services Administration (HRSA)
Within HRSA, many of the activities related to Hepatitis B and C are overseen by the HIV/AIDS Bureau (HAB) and the Bureau of Primary Health Care (BPHC). HAB and BPHC are collaborating on ways to increase screening and referral to treatment for Federally Qualified Health Center (FQHC) patients who are mono-infected with hepatitis C and those who are dually infected with HIV and hepatitis. Examples of HAB and BPHC hepatitis B and C activities include the following”:
* HRSA/BPHC is working with the Association of Asian Pacific Community Health Organizations (AAPCHO) and the White House Initiative on Asian American and Pacific Islanders to develop strategies for improving prevention and treatment of viral hepatitis among Asian and Pacific Islander Americans.
* Hepatitis C Treatment Expansion Initiative - Evaluation and Technical Assistance Center (CFDA: 93.928): Under the Special Projects of National Significance Program of the
* Ryan White HIV/AIDS program, administered by HRSA’s HIV/AIDS Bureau, this initiative will provide funds for up to 2 years to build capacity among Ryan White-funded
* organizations through the implementation of demonstration models for enhancing HCV treatment protocols in integrated HIV medical treatment settings in the context of providing HIV primary medical care and treatment to individuals co-infected with HCV. In addition to treatment implementation, awarded organizations will also assist the Evaluation and Technical Assistance Center in assessing the effectiveness, feasibility and costs of these service delivery models.
* HRSA supports FQHC services for viral hepatitis treatment and prevention in the following ways:
o Requiring that, as a condition of health center funding and the FQHC "Look-Alike" designation, all federally-funded health centers and FQHC Look-Alikes provide diagnostic lab services, screenings for communicable diseases, and immunizations against vaccine-preventable diseases, including HBV.
o Requiring that federally-funded health centers and FQHC Look-Alikes provide health education to patients and the general community. This includes patient education on diseases that may be prevalent in the community or for which the population may be vulnerable, such as viral hepatitis.
o HRSA promotes screening and treatment of viral hepatitis through a national cooperative agreement. Activities resulting from this agreement include raising awareness of viral hepatitis among health center providers and patients, and providing technical assistance on strategies to treat and prevent viral hepatitis. For example, HRSA recently met with the National Alliance of State and Territorial AIDS Directors and the Northeast Hepatitis Coordinators’ Alliance to strategize on hepatitis prevention and treatment in FQHCs.
* In order to better monitor hepatitis incidence in health center patients, HRSA revised its health center grantee reporting mechanism to track patient hepatitis rates.
* The only successful treatment available for endstage liver disease due to HCV is liver transplantation. HRSA provides oversight for the Organ Procurement and Transplantation Network (OPTN) operated under contract by United Network for Organ Sharing (UNOS). Currently there are 16,072 patients on the nationwide liver transplant waiting list, and 6.320 liver transplants were performed in 2009. Because of the critical shortage of donor organs, 1,461 patients died in 2009 waiting for a liver transplant. About 40% of liver transplants performed in the U.S. have HCV, and experts expect this number to rise significantly during the next decade. Although liver transplantation can successfully treat chronic liver failure due to HCV, a major challenge facing these recipients is recurrence of HCV in the new liver that eventually leads to reduced graft survival. 38
Food and Drug Administration (FDA)
The FDA has multiple centers working on hepatitis B and C prevention activities:
CDER Activities Relating to Hepatitis B and C: FDA’s Center for Drug Evaluation and Research (CDER) has the responsibility of reviewing drug products and certain biological products including therapeutic proteins and monoclonal antibodies for the treatment and/or prevention of viral hepatitis including hepatitis B and C.
Currently, there is a great deal of interest within industry in developing treatments for both hepatitis B and C. FDA has approved five drugs and two interferon products to treat hepatitis B. FDA has approved three distinct types of interferon products from three different sponsors for the treatment of hepatitis C. FDA has also approved multiple versions of ribavirin, a drug approved to increase the effectiveness of intereferons in the treatment of hepatits C.
CDER also regularly meets with numerous issue groups and pharmaceutical companies to discuss drug development plans, protocols and proposals. CDER is currently collaborating with the Forum for HIV Research to plan a workshop on hepatitis C drug development. FDA also held a public meeting in April 2010 to discuss expanded access to direct-acting antiviral agents for the treatment of chronic hepatitis C infection in patients with unmet medical need. CDER is in the process of drafting a guidance to industry on the development of direct-acting antivirals for the treatment of hepatitis C. And lastly, FDA issued a Citizen Petition response which recognized the crisis of hepatitis C among people with bleeding disorders and the need to take definite steps to allow people with bleeding disorders and hepatitis C and other patients with hepatitis C with no treatment options to have access to promising investigational drugs beyond current clinical trials.
CBER Activities Relating to Hepatitis B and C: The FDA’s Center for Biologics Evaluation and Research (CBER) regulates biological products for human use under applicable federal laws, including the Public Health Service Act and the Federal Food, Drug, and Cosmetic Act. CBER protects and promotes the public health by ensuring that biological products are safe and effective and available to those who need them. CBER also provides the public with information to promote the safe and appropriate use of biological products. CBER regulates an array of diverse and complex biological products, both investigational and licensed, including vaccines, blood and blood products, and human tissues and cellular products. In carrying out its mission to ensure the safety, purity, and potency (effectiveness) of biological products, CBER engages in a number of activities pertinent to HBV and HCV.
Scientists in CBER laboratories are currently working on several research projects pertaining to HCV. One research program, Hepatitis C Vaccines: Development of in vitro and in vivo Systems for HCV Replication and Evaluation of Vaccine Efficacy, seeks to evaluate new methods and models for evaluating the immune responses to HCV in systems that may be predictive of outcomes in people. Evaluating immune correlates of protection will be invaluable in the assessment of candidate HCV vaccines and to support development of new HCV vaccines.
Another research program – Studies of Efficacy, Safety and Potency Assay Development for Prophylactic and Therapeutic Vaccines against Hepatitis Viruses – is focused on developing scientific tools to understand the immunobiology and pathogenesis of HCV. Studies include the development of a small animal model for HCV infection, identification of efficacy biomarkers (i.e., immunologic correlates of protection), development of neutralization tests for the virus, use of nanotechnology for induction of protective immune responses, and studies on the safety of therapeutic vaccines for this virus. These studies will provide the ability to evaluate new technologies being applied to vaccine development, and will be pivotal in guiding and assessing the safety, efficacy and manufacturing issues associated with HCV vaccines.
CBER also engages in research activities pertaining to the safety and efficacy of plasma-derived products in the context of HBV and HCV. CBER research studies have impacted: (1) the safety of blood and blood products with respect to viral pathogens in transfusion recipients; (2) the establishment of national, international, or global standards that would ensure the safety of blood and potency of plasma-derived products; and (3) the development of cell culture based-assays to test for pathogen inactivation.
CDRH Activities Relating to Hepatitis B and C: FDA's Center for Devices and Radiological Health (CDRH), which is responsible for regulating firms who manufacture, repackage, relabel, and/or import medical devices sold in the United States, has a dedicated Office of In Vitro Diagnostic Device Evaluation and Safety (OIVD) charged with regulating all aspects of in-home and laboratory diagnostic tests (in vitro diagnostic devices, or IVDs). OIVD's multidisciplinary group of scientists, medical technologists, policy analysts, engineers, pathologists, and clinicians has a dual charge to foster the rapid transfer of new IVDs into the marketplace while preventing marketing of unsafe or ineffective devices, and is engaged in a number of activities related to hepatitis B and hepatitis C.
In addition, OIVD scientific reviewers and managers participate in several interagency groups associated with viral liver disease. The Hepatitis "Think C" Personalized Medicine Group works to improve the dosage of anti-viral medication at the individual patient level through a combination of appropriate diagnostic test and drug regimes. The Liver Fibrosis Interagency Group meets to discuss the ongoing search for new diagnostic biomarkers for liver fibrosis, which could replace the current practice of diagnosis by liver biopsy.
Indian Health Service (IHS)
IHS works to prevent viral hepatitis in its beneficiary population. IHS has a vaccination program to prevent hepatitis B in the Indian communities it serves. Routine vaccination of all newborns occurs at IHS birthing hospitals, with the first dose of hepatitis B vaccine administered as soon as possible after birth. The hepatitis B vaccine series started at birth is completed as part of normal pediatric vaccine schedule. Catch-up hepatitis B vaccination is offered to children and adolescents who need it. Vaccination of at-risk adults varies by site. Screening for the hepatitis B surface antigen in pregnant IHS patients is generally done as part of the regular health care treatment protocol. Treatment of chronic hepatitis B is provided, most notably in Alaska.
Treatment of hepatitis C occurs at some service units, with four IHS areas providing hepatitis C treatment in at least one service unit. Again, the Alaska Area offers the most developed program. The Seattle Indian Health Board Viral Hepatitis Education and Training (VHET) Project offers education and training of providers in screening of at-risk adults for hepatitis B and hepatitis C, and in hepatitis A and B vaccination. The IHS is also developing electronic health record-based surveillance methods to describe the epidemiology of hepatitis C in the HIS beneficiary population.
HHS Office of Minority Health (OMH)
OMH helped sponsor the IOM report, and is ingworking to elevate viral hepatitis as a priority public health issue. AActivities led by OMH include the following:
Hepatitis B Video, titled “B”/PSA: The OMH was asked by the Association of Asian Pacific Community Health Organizations and the Hepatitis B Foundation to collaborate on the national release of the Hepatitis “B” video/PSA. The PSA was awarded the Grand Prize of the B Real Short Film Competition at the Los Angeles Asian Pacific Film Festival in 2009 and, prior to the partnership with OMH, was played in every major feature at the Asian American International Film Festival in New York. As part of the partnership, the PSA was recently aired on ABC during the Oprah Winfrey Show, CNN’s Anderson Cooper, Good Morning America, Today Show, the evening news and various Asian media networks. The PSA will be translated into six different Asian languages.
World Hepatitis Day: The OMH, Association of Asian Pacific Community Health Organizations, National Alliance of State and Territorial AIDS Directors, and National Viral Hepatitis Roundtable recently hosted a World Hepatitis Day event to highlight the importance of global action to eliminate viral hepatitis in Asian American, Native Hawaiian, Pacific Islander, African American, American Indian, Alaska Native, and Hispanic/Latino communities.
Compendium Distribution: Compendium on Local Hepatitis B Activities: The Association of Asian Pacific Community Health Organizations (AAPCHO) received an OMH National Umbrella Cooperative Agreement to enhance hepatitis B activities in communities across the nation. As part of this award, AAPCHO will work with the Hepatitis B Foundation and Asian Pacific Islander American Health Forum to develop and implement a comprehensive strategy to promote and distribute a hepatitis B compendium to catalyze partnerships for local and national action.
The compendium includes case studies on the successes and lessons learned from local coalitions that are part of AAPCHO's hepatitis "B Activated" network. The case studies provide examples and recommendations for enhancing coalition efforts for increasing local awareness, and enhancing screening and vaccination activities. The compendium is intended for communities who are interested in developing or strengthening local hepatitis B awareness and prevention efforts.
Bilingual Bicultural Demonstration Program: Funded by OMH under the Bilingual Bicultural Demonstration Program, the Asian Liver Center at Stanford University’s “Building the Community Partnership for San Francisco: Hep B Free Campaign” works to screen, vaccinate and treat all San Francisco Asian and Pacific Islander residents against hepatitis B by providing convenient, free or low-cost testing opportunities at partnering health facilities.
Community Partnership: The Immigrant and Refugee Community Organization (IRCO), an OMH Community Partnership grantee, seeks to decrease the prevalence of hepatitis B and HIV in the Asian and Pacific Islander, African Refugee, and Immigrant communities in Portland, Oregon. Since September 2009, IRCO has reached 210 members of the Asian and African refugee and immigrant community and trained 43 healthcare interpreters on hepatitis B transmission, symptoms, and the importance of early detection.
Closing
Given the substantial and increasing disease and economic burden from viral hepatitis, HHS is taking immediate and coordinated steps to reverse these trends, which represent a health priority for our nation. HHS greatly appreciates the committee’s interest in these important issues.
Thank you for the opportunity to share this information with you. I recognize that the problems I have identified are significant ones, but I am confident that working together we can succeed in protecting this nation against the needless disease, pain, suffering, and death caused by viral hepatitis. Thank you. I will be happy to answer any questions.
1 Goldstein ST, Zhou F, Hadler SC, Bell BP, Mast EE, Margolis HS. A mathematical model to estimate global hepatitis B disease burden and vaccination impact. Int J Epidemiol 2005;34:1329--39
2 World Health Organization. Hepatitis B. Geneva, Switzerland: World Health Organization; 2000. Available at http://www.who.int/mediacentre/factsheets/fs204/en/print.html
3 W.M. Lee, Hepatitis B virus infection, N Engl J Med 337 (1997) (24), pp. 1733–1745.
4 Perz, J.F., The contribution of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. Journal of Hepatology 2006; 45 (4):529-538.
5 WHO Cancer Fact Sheet No 297 Feb 2009. http://www.who.int/mediacentre/factsheets/fs297/en/print.html
6 CDC. Hepatocellular carcinoma – United States, 2001-2006. MMWR 2010;59 (17:517-20).
7 IOM (Institute of Medicine). Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Washington, DC: The National Academies Press. At 21 (2010)
8 Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med 2006;144:705--14
9 CDC. Surveillance for Acute Viral Hepatitis – United States, 2007. 2009;58 (No. SS-3)
10 CDC. Recommendations for Identification and Public Health Management of Persons with Chronic Hepatitis B Virus Infection. 2008;57 (No. RR-8)
11 Lok AS, McMahon BJ. Chronic Hepatitis B. Hepatology2007; 45:507-539
12 Seeff LB. Natural History of Chronic Hepatitis C. Hepatology 2002; 36:S35-S46.
13 Brown RS Jr. Hepatitis C and liver transplantation. Nature 2005;436:973-978.
14 Sherman KE, Rouster SD, Chung RT, Rajicic N. Hepatitis C virus prevalence among patients coinfected with human immunodeficiency virus: a cross-sectional analysis of the U.S. Adult AIDS Clinical Trials Group. Clin Infect Dis 2002;34:831-7.
15 D:A:D Study Group. Factors associated with specific causes of death amongst HIV-positive individuals in the D:A:D study. AIDS 2010 [epublication May 6, 2010 ahead of print]
16 Altekruse SF, McGlynn KA, Reichman ME. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol 2009;27:1485--91.
17Vogt T, Wise ME, Shih H, Williams IT. Hepatitis B Mortality in the United States, 1990-2004 [Abstract]. 45th Annual Meeting of Infectious Diseases Society of America, San Diego, CA; October 4-7, 2007
18 Wise M et al. Changing trends in hepatitis C-related mortality in the United States, 1995–2004. Hepatology 2008;47:1–8.
19 CDC. Screening for Chronic Hepatitis B Among Asian/Pacific Islander Populations – New York City, 2005. MMWR 2006; 55(18):505-509.
20 CDC. Hepatocellular carcinoma – United States, 2001-2006. MMWR 2010;59(17;517-20.
21 Edmunds WJ, Medley GF, Nokes DJ, Hall AJ, Whittle HC. The influence of age on the development of the hepatitis B carrier state. Proc R Soc Lond B Biol Sci 1993;253:197--201
22 McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 1985;151:599--603.
23 Hyams KC. Risks of chronicity following acute hepatitis B virus infection: a review. Clin Infect Dis 1995;20:992--1000
24 CDC. Hepatitis B Virus: A Comprehensive Strategy for Eliminating Transmission in the United States Through Universal Childhood Vaccination: Recommendations of the Immunization Practices Advisory Committee (ACIP). MMWR 1991;40 (RR-13): 1-19. http://www.cdc.gov/mmwr/preview/mmwrhtml/00033405.htm
25 Estimated Vaccination Coverage* with Individual Vaccines and Selected Vaccination Series Among Children 19-35 Months of Age by State and Local Area US, National Immunization Survey, Q1/2008-Q4/2008† http://www2a.cdc.gov/nip/coverage/nis/nis_iap2.asp?fmt=v&rpt=tab02_antigen_iap&qtr=Q1/2008-Q4/2008
26 CDC. National, State, and Local Area Vaccination Coverage Among Children Aged 19--35 Months --- United States, 2008. MMWR 2009;58: 921-926.
27 CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: immunization of infants, children, and adolescents. MMWR 2005;54 (RR-16):1–31.
28 CDC Unpublished Data
29 JB Wong, GM McQuillan, JG McHutchison and T Poynard. Estimating future hepatitis C morbidity, mortality, and costs in the United States, American Journal of Public Health, Vol 90, Issue 10 1562-1569.
30 Milliman Study for Vertex Pharmaceuticals. Consequences of Hepatitis C Virus – Costs of a Baby Boomer Epidemic of Liver Disease. 2009
31 A Rajendra, JB Wong Economics of chronic hepatitis B and hepatitis C Journal of Hepatology, 2007 Oct: 47 (4):608-17. Epub 2007 Jul 30
32 Kanwal F, et al., Treatment alternatives for hepatitis B cirrhosis: a cost-effectiveness analysis. The American Journal of Gastroenterology, 2006;101(9):2067-2089.
33 Spackman DE, Veenstra D. A cost-effectiveness analysis of currently approved treatments for HBeAg-positive chronic hepatitis B. PharmacoEconomics, 2008;26(11):937-949.
34 Wong JB, et al., Cost-effectiveness of interferon-alpha 2b treatment for hepatitis B e antigen-positive chronic hepatitis B. Ann Intern Med, 1995;122(9):664-675
35 Hutton DW, Tan D, So SK, et al. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med, 2007;147(7):460-469.
36 Licata A, DiBona D, Schepis F, Shahied L, Craxi A, Camma C. When and How to Treat Acute Hepatitis C? J Hepatol 2003;39:1056-1062
37 CDC. Implementation of Newborn Hepatitis B Vaccination – Worldwide, 2006. MMWR 2008;57(46):1249-1252.
38 TD Schiano and P Martin, Review: Management of HCV infection and liver transplantation, International Journal of Medical Sciences (2006) 3(2):79-83.
Last revised: September 09,2010
Subscribe to:
Comments (Atom)